General information
The skin of a newborn, on the one hand, is a protective barrier, and on the other, the most vulnerable organ. This is due to the fact that the barrier is easily destroyed under the influence of unfavorable factors (damage, chemical exposure, background conditions, defects in care). The skin is very vulnerable due to its immaturity and structural features. The epidermis is loose, and the stratum corneum is thin, so it cannot fully provide protection. As for premature babies, the barrier function is formed only by the end of the child’s first month. Elastic fibers of the skin, which protect against damage, are formed by two years. In this regard, the skin easily macerates (“looses”) at the slightest impact. Due to defects in care (infrequent diaper changes, poor cleaning), traumatic damage and friction, diaper rash often occurs (medical term diaper dermatitis ).
Diaper rash is a non-infectious inflammation of the skin that has been subjected to friction or prolonged contact with moisture. Local inflammation is localized in the folds, buttocks, perineum, and abdomen. The degree of inflammation can vary from mild redness to weeping areas with cracks and erosions. This pathology occurs in children under one year of age and is more common in girls. The incidence of diaper rash is lower in infants who are breastfed. This is due to the less acidity of feces and urine. After 1.5 years, the incidence is lower, which is associated both with the “ripening” of the skin and with the fact that the child may ask to use the potty.
A type of diaper rash is intertrigo (intertriginous dermatitis) - an inflammatory process of skin folds. The most common causes of lesions in skin folds are opportunistic fungi, bacteria and bacterial-fungal mix. This pathology occurs in adults, who, to a greater extent than newborns, have contact with bacterial and fungal pathogens.
Diaper dermatitis in children: how can we cope with it?
Both pediatricians and parents of young children consider diaper dermatitis one of the most common skin diseases. Almost every child experiences this condition to varying degrees of severity during the first months or years of life [1, 2]. Diaper dermatitis is diagnosed in 7–35% of infants, with peak prevalence at 9–12 months of age. life regardless of gender and race [3]. According to a study of the prevalence of skin lesions in the intensive care unit of the Children's Hospital of Philadelphia in 2008, diaper dermatitis was detected in 24% of inpatients [4]. This high frequency is largely due to the skin characteristics of young children.
Research in recent years has made it possible to obtain new information about the skin, explain its inflammatory response and justify the use of skin care products to prevent this condition. The skin as an organ is represented by the epidermis, the dermis itself and skin appendages. The skin is a dynamic system with the ongoing process of proliferation of keratinocytes in the basal layer of the epidermis, desquamation of corneocytes on the surface of the skin, and degradation of dense ligaments of corneodesmosomes [6]. In the apical layer of the epidermis, the stratum corneum, corneocytes are organized into an intercellular lipid matrix of laminar bodies consisting of cholesterol, ceramides and free fatty acids [7].
Details of infant skin morphology, such as surface structure, skin thickness, and cell size, have been visualized microscopically and calculated using computer analysis of microscopic images and skin impressions in silicone and adhesive tapes [8–10]. Video microscopy and in vivo confocal laser scanning microscopy make it possible to 3D image the topography of the skin and the internal structure of the dermal layers [9]. The results of these in vivo studies have expanded our understanding of children's and adult skin and articulated their differences.
The skin performs many different vital functions. Among them are physical and immunological protection from the damaging influences of external environmental elements (including microorganisms, ultraviolet radiation, humidity, extreme temperatures), sensory perception (pain, temperature, touch), temperature regulation, water and electrolyte homeostasis, gas exchange.
Understanding the physiology of normal healthy infant skin (the point of comparison) is important from a clinical perspective. Clinical studies on healthy infants, however, are ethically limited (in relation to the use of invasive methods), so they are few. New non-invasive technologies for measuring electrical capacitance, transdermal water loss, and absorption-desorption rates in infants and adults [10] have shown differences in skin barrier function, revealing dynamic changes in the level of natural hydration factor and water profile of the skin of infants, young children and adults [11] .
The structure, functions and constituent elements of infant skin differ from those of an adult organ - primarily in that during the first year of life and somewhat longer, a continuous maturation process continues in the skin. The epidermis of newborns is completely differentiated. In children of the first year of life and early age, corneocytes and granulocytic cells in the epidermis differ from those in adults in smaller size (by 20 and 10%, respectively) and in number [5]. The stratum corneum and epidermis of infant skin are 30 and 20% thinner than adults, respectively [5]. Microrelief lines are denser in children, while the depth of surface glyphs in children is similar to that in adults [5]. There is less melanin in the epidermis of children [12]. The dermal papillae, their density, size, and morphology are more homogeneous in children than in adults [5]. In children, there is no clear boundary between the papillary and reticular layers of the dermis [5]. In the components of the epidermis in infants, the concentration of natural moisturizing factor is lower than in adults [10]. It is important that children have higher skin pH values than adults, with the highest pH levels in newborns [13]. The level of surface skin lipids and sebum in children is lower than in adults [14], and the water content in the stratum corneum in infants is higher [11]. The density of collagen fibers in the dermis of children is lower than that of adults [5].
The listed features of the structure and composition of the skin determine the uniqueness of its function in children. Newborns have drier skin than adults, but during the first month of life the picture completely changes. In children 3–24 months. life, there is increased skin hydration compared to adults. The barrier function and moisture of the skin are also related to the intercellular lipid matrix, a natural moisturizing factor and the passage of water molecules through the stratum corneum. The rate of water absorption and desorption in the skin is higher in children than in adults, as is transepidermal water loss [10].
In addition to structural and functional changes, the composition of the skin microflora forms and changes in the first year of life. The predominant microbes on infant skin are Firmicutes (mainly Staphylococci), followed by Actinobacteria, Proteobacteria and Bacteroidetes. In adults, the phylum Proteobacteria dominates, followed by Actinobacteria and Firmicutes [15]. How to apply these research data is currently not entirely clear. Early microbial colonization may influence the development of skin immune function. The barrier function is vital for survival, preventing pathogens from entering the body. If the skin barrier is damaged, bacterial factors gain access to epidermal keratinocytes and can induce a protective immune response. Keratinocytes produce antimicrobial peptides. In the absence of these proteins, pathogenic microorganisms can invade the skin, disrupt the commercial/pathogen balance, or lead to infection.
The morphological characteristics of infant skin determine its easy vulnerability. Increased humidity, insufficient function of the sweat glands, and abundant vascularization of the skin can contribute to the rapid development of certain pathological conditions, such as irritant contact dermatitis and inflammatory processes.
Diaper dermatitis is common in young children. Diaper rash affects the lower abdomen and back, buttocks, perineum, and inner thighs. Wearing diapers causes an increase in moisture in the skin and an increase in pH (alkalinization). If high humidity persists for a long time, softening and loss of integrity of the skin (maceration) may occur, making it more susceptible to friction from the surface of the diaper. It also increases the risk of further skin damage and problems caused by exposure to other irritants, particularly feces containing proteases and lipases and ammonium in the urine. Other factors that can worsen the condition and worsen the rash include repeated washing and cleansing of the skin, inadequate skin care, infections, antibiotics, diarrhea and bowel and urinary tract problems [16].
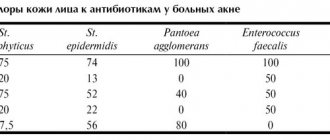
Diaper dermatitis manifests itself as a rash in the diaper area (when diagnosing, other causes of rash in this area should be excluded) (Table 1). It is also necessary to take into account and evaluate the following factors (Table 2):
1. Hygiene skills (for example, how often to wash a child, change a diaper). Poor hygiene and prolonged contact with urine/feces predispose to irritant dermatitis.
2. Type of diapers used - disposable or reusable cotton.
3. Use of irritant products for washing and cleansing the skin, such as soaps, detergents, wet wipes with fragrance/alcohol.
4. Skin trauma: for example, diaper friction, excessive washing with vigorous cleansing.
5. Recent use of antibiotics, which predisposes to Candida colonization and diarrhea.
With diaper dermatitis, there is usually redness of the skin in the area covered by the diaper (buttocks, perineum, pubic area, upper thighs), with no redness in the deepest skin folds. The skin may have a slight shine, mild flaking, and hypopigmentation. The rash usually does not cause other symptoms until it becomes severe or painful. Mild diaper dermatitis involves a faint, pink rash covering less than 10% of the diaper area, with or without occasional scattered papules, slight sheen, and dryness. A mild course, as a rule, does not cause concern for the child and can usually be stopped with simple care measures. Moderate/severe course involves moderate to severe hyperemia, occupying an area of more than 10% of the skin under the diaper, with or without the presence of papules, spots, swelling or ulceration. With this degree of severity, irritability of children is noted, secondary infection with Candida albicans is determined, and often stomatitis. The erythema expands to areas outside of contact with feces, the diaper, and develops into confluent lesions with distinct edges with papules, pustules, involving the skin folds of the area of skin in contact with the diaper. Associated injuries and stomatitis are typical [17]. Signs of a bacterial infection include redness with exudate, blisters, small blisters, and pustules. If the rash in the diaper area is severe or does not disappear despite treatment, or there is doubt about the diagnosis, you should consult a dermatologist and conduct additional examination.
Relieving diaper dermatitis requires good child care, ongoing skin assessment, and parent education. Caring for the diaper area includes:
1) reducing the interval between changing diapers;
2) changing the diaper after soiling;
3) use of modern diapers;
4) cleansing the perineal area - by washing with warm water and emollient or wiping with wet wipes without alcohol and fragrances;
5) use of a water-repellent emollient or barrier agent after each diaper change to reduce irritation from contact with urine and feces;
6) air baths after washing [18].
In most cases, diaper dermatitis can be successfully treated with the above measures. If this is not enough, in moderate cases, topical corticosteroids and topical antifungals may be prescribed, applied to the skin under a barrier drug.
If candidal lesions are suspected, nystatin, clotrimazole or ketoconazole, miconazole are most often used. To reduce inflammation, if dermatitis persists, weak steroids, hydrocortisone, are prescribed [19]. Basically, 0.5–1% hydrocotisone is used, applied until the skin is cleared of the rash, but not longer than 1 week. Damaged infant perineal skin in a warm, humid environment has enhanced percutaneous absorption of drugs. In the USA, medium and strong steroids are used, often in combination with antifungal components (nystatin - triamcinolone, clotrimazole - betamethasone dipropionate) [19]. However, due to possible side effects for mild and moderate dermatitis in pediatric practice, their use should be avoided [20]. If dermatitis is complicated by a secondary infection (bacterial), then topical antibacterial drugs are used [21]. When choosing treatment tactics for dermatitis, you should be guided by scientifically based recommendations and the results of clinical studies.
Diapers. There are different types of diapers available today. The development of superabsorbent polymers has made it possible to produce new thin materials with a gel layer, which are currently used in diapers. New products are characterized by an increased rate of capture and absorption of liquid, high moisture capacity, which makes the skin surface drier. Diapers are created for babies of different ages, taking into account physiological characteristics. But at present, clinical studies do not provide sufficient evidence that certain types of diapers can be used to prevent diaper dermatitis [22].
The use of soaps and lotions is not recommended for cleansing the skin. Their use changes the pH of the skin, leading to greater dryness and damage [23]. A recent study found that using alcohol- and fragrance-free wet wipes was as effective at cleansing and hydrating the skin without damaging the skin as bathing in water using a cloth skin cleanser [24].
Barrier products create a protective layer between the skin and feces. The ideal barrier product should be one that has proven effectiveness in children and works similarly to the skin's natural function, forming a long-lasting barrier to maintain optimal moisture levels. It should not contain unnecessary ingredients, irritants, toxic ingredients or ingredients with undocumented safety [18]. However, there is insufficient evidence that barrier cream is more effective in the treatment of uncomplicated diaper dermatitis than simple water-repellent ointments (vaseline, paraffin) [16]. Water-repellent emollients or barrier preparations are applied at every diaper change. They form a protective lipid film on the surface of the skin and thereby protect against irritation upon contact with feces. Most products contain zinc oxide, petrolatum, or both. Under this layer, damaged skin is protected from irritation, healing occurs, and there is no excess skin moisture [25].
Barrier creams also use other ingredients, such as cod liver oil, aloe, dimethicone, and dexpanthenol [26]. In some European countries, a 2% aqueous solution of eosin is used to treat diaper dermatitis [27]. The absence or deficiency of barrier creams is associated with relapses of diaper dermatitis [28]. Barrier preparations may contain antiseptics and fragrances. Zinc preparations and castor oil may contain parts of peanut (groundnut) oil. Children with allergies to nuts and soy should not use such products. Ointments and creams containing vitamin A, calendula, honey, tea tree, recommended for the prevention and treatment of diaper dermatitis, do not have a sufficient evidence base of effectiveness. More research is needed.
To heal the skin and restore its protective properties, rapid regression of clinical manifestations of diaper dermatitis, positively proven topical dermato-reparative drugs, in particular Bepanten ointment, should be prescribed. The active principle of these drugs is dexpanthenol (provitamin B5). Pantothenic acid is a vital component of normal epithelial function. It is a component of coenzyme A, a cofactor for various reactions in the metabolism of carbohydrates, fatty acids, proteins, gluconeogenesis, steroid hormones, and porphyrins.
Dexpanthenol has been well studied. By the end of the twentieth century. Many works have been published that have proven its effectiveness in dermatology. A review of German researchers [29] summarized data from 56 publications. The use of dexpanthenol is based on its good penetration and high local concentration in the skin when used in the appropriate form, in particular as a water-in-oil emulsion. Topically, it acts as a humectant, improving hydration of the stratum corneum, reducing transepidermal moisture loss, maintaining skin softness and elasticity.
In vitro and in vivo studies revealed the effect of dexpanthenol on the activation of fibroblast proliferation, and accelerated reepithelialization during healing of the wound surface was proven. The anti-inflammatory effect of dexpanthenol was demonstrated in an experimental model of ultraviolet-induced erythema. Beneficial effects of dexpanthenol have been revealed in patients with skin grafts, in the treatment of scars, burn injuries, and various dermatoses. The most significant effects of dexpanthenol were stimulation of epithelialization, granulation and reduction of itching.
Double-blind, placebo-controlled studies assessed the effectiveness of dexpanthenol in wound healing. A decrease in erythema and more elastic and durable tissue regeneration have been shown in the treatment of epidermal wounds with dexpanthenol emulsion compared to treatment without its use. Monitoring of transepidermal water loss showed a significant acceleration of epidermal regeneration as a result of dexpanthenol therapy compared to placebo. In an experiment on a model of irritation, in the group that used dexpanthenol cream before irritation, significantly less damage to the stratum corneum barrier was detected compared to that in the group that did not use this drug. Skin care with dexpanthenol significantly improved symptoms of skin irritation such as dry skin, roughness, flaking, itching, erythema, erosions/cracks after 3-4 weeks. Usually, dexpanthenol preparations are well tolerated, the risks of irritation or hypersensitivity are minimal [29].
Of interest is a prospective observational study to evaluate the effectiveness of self-administered ointments containing dexpanthenol in treating irritated skin [30]. The study was conducted in Germany by pharmacists at a network of 392 pharmacies and included 1,886 patients with symptoms of irritated skin, including non-acute atopic eczema, as well as other conditions with skin xerosis and a damaged skin barrier. Efficacy assessment was carried out on the 7-10th day after treatment with calculation of the therapy effectiveness index / economic benefit. As a result, 91.5% of patients noted the benefits of therapy, 94.7% directly indicated the success of treatment. All symptoms of irritated skin (xerosis, erythema, desquamation) decreased significantly. There were no differences in responses depending on age, gender, or skin diseases. A high index of therapeutic effectiveness/economic benefit has been shown in the treatment of irritated skin with dexpanthenol ointment.
In the last decade, the volume of data on the protective effect of dexpanthenol has expanded. Thus, in a double-blind, placebo-controlled study, its effectiveness in protecting against irritation [31] and in the treatment of diaper dermatitis in infants was proven [26]. A multicenter study demonstrated the effectiveness of 5% dexpanthenol and zinc oxide ointment in the treatment of irritant diaper dermatitis in diarrheal syndrome in children [32].
Dexpanthenol is registered in Russia in the pharmacological group of regenerants and reparants. The results obtained in a number of clinical studies led by N. A. Korovina et al. (2004), V. A. Revyakina (2004), Yu. S. Akoeva et al. (2005), indicate the high clinical effectiveness and tolerability of Bepanten ointment (5% dexpanthenol) in the treatment of children with diaper dermatitis. It was found that in most cases, already on days 2–3 of therapy, there was a decrease or disappearance of clinical manifestations on the skin. It should be especially emphasized that among the subjects studied there were not only infants, but also newborns (both full-term and premature). At the same time, the positive effect of Bepanten was noted when used both in newborns and older children [33].
We present a clinical case of diaper dermatitis.
Girl E. Age 1 month. 5 days. During a routine examination by a pediatrician at the age of 1 month. Mom reported to the doctor about a rash in the diaper area on the 2nd day. Hereditary history is aggravated on the maternal side: my grandfather has allergic rhinitis and asthma during the grass flowering season, and my older sister has allergic rhinitis during the tree flowering season. The girl is the second desired child in a prosperous family; from the 2nd successful pregnancy with mild nasopharyngitis suffered without the use of drugs at the 6th month, timely physiological birth at 40 weeks. She was born with a weight of 3940 g, height 53 cm, chest circumference 35 cm, head circumference 35 cm. Apgar score - 8 points. She screamed immediately. They put me to the breast in the delivery room. In the early neonatal period, toxic erythema was noted. Vaccinated according to the calendar without complications. Psychomotor development by age. Breastfed girl. In the first month I gained 950 g of weight.
At the age of 14 days there was a single episode of skin hyperemia in the diaper area. Mom explained this by saying that she had not calculated her urine output that day and was late in changing the diaper. The hyperemia went away within a day when the diaper was changed; no doctor's consultation was required. The mother bathed the child with baby soap and used baby cream. After this episode, I began using body foam when bathing. The 2nd episode of rash at one month of age was associated with the fact that the child’s stools became up to 7 times more frequent with a sour smell, which caused skin irritation. Mom assumed that this was a response to the excessive amount of fried potatoes she had eaten the day before. The stool was restored after 1 day. The girl's behavior, sleep, and appetite have not changed. At the pediatrician's examination, the child is calm. The child's general condition does not suffer.
Objectively: locally on the skin of the perineum, pubic area, upper third of the inner thighs, buttocks against the background of moderate hyperemia, papular elements. Deep folds are not involved. There is no itching.
In a general blood test at the age of 1 month: hemoglobin - 132 g/l, erythrocytes - 4.0 × 1012, color index - 0.9; leukocytes - 8.2×109; eosinophils - 2, band neutrophils - 2, segmented neutrophils - 18, lymphocytes - 74, monocytes - 4, ESR - 4 mm.
In the coprogram: consistency - mushy, color - yellow, smell - fecal, mild, pH - slightly acidic, mucus was detected; no blood or undigested food was found. Microscopic examination of stool: mucus - moderate, leukocytes - 0-5 in the mucus, no other ingredients were detected.
Diaper dermatitis was diagnosed. Advice is given on rational nutrition for a nursing mother and keeping a food diary. For skin care, Bepanten ointment is recommended after each diaper change. Examination after 5 days showed a positive effect with the restoration of pink, clear skin and satisfactory condition.
In this case, diaper dermatitis occurred in a child with a high risk of developing allergic diseases. Early onset in the first month of life indicates the vulnerability of the skin. Episodes of its damage can serve as a trigger for the development of inflammation, including allergic inflammation. Restoring the integrity and function of the epidermal barrier is protective against the development of chronic pathology. Long-term use of Bepanten ointment to preserve the integrity of the skin in this case is justified.
Thus, it is necessary to emphasize that new data on the morphology and function of the skin in different periods of its maturity at different ages make it possible to reveal the mechanisms of its damage and create the necessary skin care products. Diaper dermatitis is a common inflammatory skin reaction in infants. The diaper, covering the skin surface, creates conditions for external environmental influences that contribute to skin irritation, which begins with damage to the skin barrier caused by components of urine and feces. Maintaining the integrity of the skin barrier with protective creams along with frequent diaper changes is an effective preventative strategy.
Pathogenesis
The pathogenesis of diaper rash is associated with the influence of a number of damaging, predisposing and provoking factors. The main role is played by a combination of chemical (stool enzymes, urine products), mechanical (friction) and microbial (from feces and urine) damaging factors against the background of impaired skin care and a decrease in its protective function.
Prolonged contact with moisture increases the moisture content of the skin, which increases friction against the diaper (moisturized skin is easily damaged by friction). Enzymes (enzymes) of feces irritate the skin, cause loosening of the epidermis and increase its permeability. Urine enhances the aggressive action of fecal enzymes. The incidence of diaper rash is lower in infants who receive breast milk because the intestines of infants who drink cow's milk contain urease-producing bacteria. An increase in skin moisture and a shift in pH to the alkaline side contribute to the proliferation of Candida albicans and bacteria, so inflammation “under the diaper” intensifies. The activity of fecal enzymes increases with diarrhea, so diaper dermatitis is very common in babies with bowel movements.
Treatment with folk remedies
It is not recommended to engage in such healing. Grandmothers advise using starch as a powder. However, it tends to harden and form into lumps. This causes the skin to suffer even more. Starch also feeds bacteria and promotes their proliferation.
If you notice the first appearance of redness, you should consult a doctor. He will conduct an examination, identify the cause of the disease, and prescribe a course of treatment for the disease. The task of every mother: attentive care, timely procedures, nutrition of the baby. There are times when, in addition to a visit to the pediatrician, you will need to be examined by an allergist.
If you want to protect the crib from baby feces, do not cover it with ordinary oilcloth, buy one with a fabric base. It will prevent the skin from chafing.
How to cure a baby from diaper rash without medications? This disease is unpleasant. Mom is irritated by the tears and whims of the baby. Urine entering the folds of the skin causes pain. If the disease is not properly treated in time, it can eat away large areas of the skin.
Based on everything stated above in this article, we can highlight the following recommendations for curing this disease in infants.
Diapers. When the first symptoms of diaper rash and redness appear, you should immediately stop using diapers. Such actions will slow down the development of pathology. The first symptoms of the disease will go away immediately.
Bathing. After taking water procedures, the baby should be thoroughly dried and lubricated with oil containing panthenol. It is recommended to apply powder to the perineal area. It is best to avoid using baby cream on lesions.
Cloth. Washing children's underwear with aggressive detergents is strictly prohibited during illness. Better switch to using baby soap. Don't forget to iron baby clothes on both sides. Buy clothing items only from natural fabrics. No rough seams on the pants.
Air. During the changing period, give your baby time to lie in the air. Air baths are very beneficial. They prevent the appearance of skin moisture and prevent inflammatory processes from arising.
Hygiene. When you see that the baby is fussing, check the diapers and rompers. It is very important to prevent the baby from coming into contact with urea at the first signs of diaper rash. During periods between urinations, you can use anti-allergy wipes to wipe the baby's skin.
In the evenings before bed, bathe your baby with the following herbs:
- chamomile;
- linden;
- successions.
A small amount of potassium permanganate will reduce the risk of infection getting to the affected area of the skin.
After eliminating diaper rash, do not relax. The baby’s folds must be looked after even after recovery from the disease with the same regularity and attention. However, instead of medicines, use creams, powders, and oils. During the hot season, do not put diapers on your baby. Let the body breathe.
You should always remember: it is easier to prevent any disease than to treat it. Therefore, ensure that all hygiene standards are observed. With proper care, diaper rash on an infant's bottom will not appear or will quickly disappear.
In children, inflammation often occurs on the skin under the influence of heat, moisture and friction. Most often, diaper rash occurs on the bottom of a newborn; there are cases of their appearance in the armpits, inguinal folds, and neck. There are quite a lot of factors that provoke inflammation of the skin on the butt; to eliminate the problem that has arisen, it is important not only to start treatment on time, but also to determine the cause of its occurrence.
Diaper rash on the butt in children is a common occurrence, and not least because of the children’s adaptation to environmental conditions.
Classification
There are:
- Primary diaper dermatitis.
- Secondary.
Primary can be complicated or uncomplicated. Uncomplicated - a consequence of improper care, skin characteristics or metabolic processes (for example, ammonia irritation). If we consider the complicated form, it develops when a fungal, bacterial and viral infection accumulates. Secondary diaper dermatitis is observed in allergic skin diseases.
Severity of diaper rash (they develop sequentially):
- A mild degree is manifested by hyperemia (erythematous diaper rash) on the buttocks, lumbar region, genitals, and abdomen. Erythematous diaper rash is associated with increased sweating and the action of irritating factors on the skin. Without treatment, inflammation progresses.
- In moderate cases, microcracks, erosions, small ulcers (pustules) appear, and infection occurs with streptococcus or candida fungus. Yeast diaper rash has a shiny, bright cherry-colored surface and a vesicular rash along the periphery.
- If there is a severe degree (severe diaper rash), then this is always a process complicated by infection. Deep erosions, ulcers and widespread infiltrates occur, and the epidermis exfoliates along the periphery with large scalloped outlines. In the depths of the folds there are non-bleeding cracks. Streptococcal diaper rash is characterized by intense weeping and the appearance of continuous erosion. The secondary inflammatory process occurs with intoxication and fever. An extreme manifestation of severe disease is microbial eczema .
Diaper rash in the groin in men is as common as diaper rash in the groin in women. A high incidence of intertrigo is observed in individuals suffering from diabetes , autonomic neurosis and obesity . sweating and immunodeficiency contribute to this condition . The growth of mycoses in hot weather is associated with high temperature and humidity, wearing synthetic clothing that does not allow air to pass through and does not absorb moisture. With this disease, maceration and cracks form not only in the groin, but also in the intergluteal fold, armpits and under the abdomen.
Should I take my child to the pediatrician?
If you have any doubts or concerns, visit your pediatrician . Especially if diaper rash is severe, the child is restless.
Young, inexperienced mothers worry about every little thing, and even a slight blush can scare them. Therefore, you can call a doctor or nurse to your home, they will examine the baby and make appointments.
If the process goes further, irritation becomes weeping, cracks appear - call a doctor immediately. Remember that this is serious suffering for the baby, and you may be doing something wrong.
Causes
The reasons are:
- violations of hygienic care (poor skin care, refusal to bathe, untimely change of diapers);
- mechanical and chemical effects on the skin;
- increased skin moisture and lack of aeration;
- low quality diapers and clothes;
- background conditions ( atypical dermatitis , seborrheic dermatitis ).
Contribute to the development of diaper rash:
- age-related skin characteristics;
- change of feeding (switching to artificial);
- taking antibiotics ;
- intestinal disorders;
- teething;
- excessive wrapping;
- high temperature in the room;
- inappropriate diaper size (small and tight-fitting).
Features of care
First you need to rule out the cause of diaper rash. Perhaps you rarely change his diapers, or don't let him lie naked . Perhaps the baby is wearing tight underwear or his clothes have become too small for him.
Pay attention to the air temperature in the room, and see if the baby is wearing too many layers of clothing.
Also, caring for a child with diaper rash should be as follows:
- Proper hygiene - after each bowel movement, the baby should be washed with warm water, and after bathing, he should be dried with disposable paper towels.
- Air baths - after any washing, the affected skin should be “ventilated” for at least 20 minutes; if contact with air is frequent, diaper rash will go away much faster.
- Caring for children's clothes - you need to wash baby's clothes with a specially designed powder, at high temperatures, it is recommended not to add softeners, it is better to iron the clothes on both sides.
- The baby's clothes should be made from natural materials ; if it is warm, let the baby sleep with his bottom bare.
- Good nutrition - the baby will recover faster if the mother eats properly and nutritiously, and, consequently, the baby’s body receives all the important vitamins and minerals.
It may be worth changing the brand of diapers. During treatment, you can safely take a larger diaper; the child should be comfortable, it should not fit too tightly.
Symptoms
It should be noted that after minor signs of irritation appear, diaper rash in newborns quickly progresses if measures are not taken to eliminate the provoking factors. A severe form in a child, in which treatment under the supervision of a doctor is required, can develop very quickly (in 1-2 days).
What does diaper rash look like in newborns?
If the diaper does not absorb urine enough, diaper rash appears in the groin of newborn boys, since the skin is constantly wet. In children with sensitive skin or prone to allergic reactions, irritation appears on the bottom, perineum and genital area. The likelihood of its occurrence increases if the diaper is rarely changed. This is due to the fact that when overfilled, the absorbent properties of the diaper are reduced. Redness under the arms develops when the child sweats and the delicate skin rubs against rough parts of clothing. Foci of redness have clear boundaries, and the color intensity can range from pink to bright red. Lack of care and treatment causes progression of the process - the development of superficial ulcers. It is assumed that if redness persists for three days and does not respond to treatment, the skin is infected with Candida fungi or bacterial flora.
If we consider this process in stages, then at the beginning (first stage) the irritability of the skin increases - slight and faint local redness appears.
Photo of erythematous dermatitis
In the second stage, if irritating factors are not eliminated, the skin appears bright red (inflammation), and erosions and cracks appear on the surface of the skin. Microorganisms found in feces infect the baby's irritated skin. When a microbial infection occurs, the surface becomes wet (weeping), bright red, and against the background of hyperemia, microcracks, ulcers and pustules appear. The elements spread quickly, forming large areas of skin damage.
The lesion has clear boundaries, swelling . The eroded surface may contain purulent (with a bacterial infection) or white cheesy (with a fungal infection) coating. A pustular rash may appear around diaper rash due to a bacterial infection. Such complications are accompanied by itching, pain and burning. In some cases, the temperature rises, the child is restless, cries, does not sleep, and refuses to eat. Complicated diaper rash is severe and long lasting.
How to treat diaper rash on the bottom of newborns?
If it is not possible to protect the baby from such a reaction of the body, mandatory treatment is required. The baby's condition will worsen if no attention is paid to this phenomenon. Fungal diseases may appear, and various types of infections can enter the body.
If there is slight redness of the skin, medicinal intervention will not be needed. In such cases, only proper care is needed, then treatment of diaper rash on the bottom of newborns can be avoided.
What should a mother's actions be:
- change diapers promptly;
- makes sure that the baby’s bottom is always dry and clean;
- It is strictly prohibited to leave a child in wet diapers. They change every three hours;
- in the process of changing clothes, the butt is washed and dried. It is better to dry for 15 minutes in the air. Then lubricate the baby's skin with cream.
Redness of the skin can be caused by the diaper itself. This indicates the need to use diapers from another company.
If all hygiene rules are followed, but diaper rash does not go away, on the contrary, it increases, cracks appear, you should consult a doctor. After the examination, he will find the reasons for this reaction and help with treatment.
Prevention
The immaturity of the baby's skin requires careful care, which is the prevention of diaper rash and all kinds of skin rashes. Proper skin care includes:
- the use of modern products for child skin care (children's cosmetics include liquid soap, baby soap with neutral pH, cream, lotion, oil);
- Frequently washing the child after defecation and urination with thorough drying of the skin;
- eliminating friction on the skin of diapers, clothes and nappies;
- correct choice of diapers by size (weight);
- frequent diaper changes - after each feeding, before bedtime, during the night, after a night's sleep;
- use of diaper cream (Bubchen, Mustela1 2 3, Bepantol);
- refusal of baby powder;
- use of intimate hygiene wipes (Pampers, Huggies, Johnson's Baby), which clean, moisturize and maintain pH balance.
Food intolerance
Lactase deficiency, when a child does not have enough lactase enzyme, which digests milk carbohydrates, is also accompanied by the occurrence of diaper rash. With this disease, the stool is loose, frequent and has an acidic reaction, which is very harmful to the child’s skin.
The occurrence of diaper rash may be accompanied by food allergies. In this case, most likely, skin redness and rashes will be not only on the skin under the diaper, but also on the cheeks, behind the ears, etc. The appearance or increase in diaper rash will coincide with the consumption of an allergenic product by a child or a nursing mother.
Consequences and complications
- Maceration and weeping ;
- formation of ulcers ;
- infection of subcutaneous tissue and skin - purulent complications are caused by staphylococci and streptococci (purulent infiltrates, impetigo and abscesses are not excluded), and Candida fungi - candidiasis ;
- itchy skin can cause disorders of the nervous system;
- Diaper rash in skin folds (under the arms, in the perineum, groin) in men and women in hot conditions contributes to increased growth of microorganisms and the development of folliculitis (purulent inflammation of the hair follicle).
In what places is the skin most often affected?
There are places on the human body that are traditionally susceptible to the development of this pathological process. The locations of diaper rash are similar in a child and an adult. Here they are:
- skin folds on the neck, arms and thighs, less often the skin is affected in the folds on the back;
- places under the mammary glands and between them, a fold under the overhanging fat layer on the abdomen;
- in the armpits of an adult or child, where in addition to sweat and lack of ventilation, the skin is also subject to friction when moving the hands;
- in the groin and between the buttocks, diaper rash appears for the same reasons as in the armpits.
List of sources
- Ryumina I.I. Prevention and treatment of diaper dermatitis in a neonatology hospital / Issues of modern pediatrics / 2015/ VOLUME 14/ No. 2.- p. 298-299.
- Garina S.V., Soldatova O.N., Tumaeva T.S., Balykova L.A. Modern ideas about the mechanisms of occurrence and approaches to the treatment of diaper dermatitis // Attending physician. — 2014. -No. 5.
- Koval G.S. Prevention and treatment of diaper dermatitis // Issues of modern pediatrics, 2004, vol. 3, no. 5, pp. 60-64.
- Studenikin V.M., Studenikina N.I. Diaper dermatitis: prevention, treatment, extradermal aspects / Attending physician. - 2009. - No. 3.
- Zaplatnikov A.L. Prevention and treatment of diaper dermatitis in children // Current issues in the development of children. 2008.No. 4. P. 24.
Fisenko Karina Olegovna
Specialty: Adult gynecologist, gynecologist-endocrinologist Work experience: more than 25 years Cost of appointment: 1600 rubles Cost of online appointment: 1200 rubles
Make an appointment
- Clinical picture of the disease
- The main causes of inflammation of the external genitalia and vagina in children
- Types of vulvovaginitis in girls
- Diagnosis of the disease
- Treatment of the disease
Prohibited manipulations
When treating an infant's diaper rash, parents independently decide to use medications, thereby making a mistake. Common misconceptions:
- Self-medication. It is necessary to show the baby to the doctor when the first signs appear, at an early stage. Treating an advanced process is more difficult than the initial manifestation.
- Baby powder. There is no need to use it to eliminate diaper rash; it will only worsen the situation. The powder is good to use for preventive purposes, applied to healthy skin.
- Starch. Replacing powder with starch to dry diaper rash is strictly prohibited. Starch tends to harden when rolled. Hard pellets rub the already damaged skin.
- Wet wipes. Under no circumstances should they replace water. You can use napkins for hygiene procedures only as a last resort.
Return to contents
What examination and when is carried out for atresia of the anus and rectum?
If any signs of intestinal abnormality are detected, an examination is carried out, including:
- An X-ray examination of the abdominal cavity shows where the rectum ends and allows us to understand whether there is an anomaly in the development of the lower parts of the spine;
- Ultrasound examination (ultrasound) of the abdominal cavity and retroperitoneal space shows disturbances in the outflow of urine from the kidneys and bladder or abnormalities in the structure of the kidneys;
- Ultrasound examination of the spine performed during the first 3 months of life allows us to evaluate deformations and accretions of the spinal cord, which can lead to subsequent neurological disorders during growth. If ultrasound reveals abnormalities in the structure of the spinal cord, then magnetic resonance imaging (MRI) of the spine is performed. After 3 months, the information value of ultrasound for assessing the spinal cord decreases;
- Echocardiography to detect heart defects.
How to treat irritation from diapers with allergies
If the cause of rashes and redness is an allergy to diapers, then you should immediately stop using them and switch to another brand. Having selected diapers that do not cause allergies in your baby, it is better not to experiment with manufacturers and stick to this brand. It is not necessary to choose the most expensive diapers: the main thing is that they provide high-quality moisture absorption and are suitable for the child.
In case of severe allergies, the child will be prescribed internal or external antihistamines approved for infants. They will speed up the relief of symptoms and quickly reduce pain, redness and itching.
How to treat diaper irritation due to fungus
Irritations caused by the fungus are easily treated in the first stage and difficult to treat in an advanced form. Antifungal ointments and creams that are applied to previously washed and dried skin help get rid of the fungus. In case of advanced infections, the child may be additionally prescribed internal medications, which have a lot of side effects. You should not treat the fungus yourself: contact your pediatrician, who will select medications that are as safe as possible for the child.
ethnoscience
Traditional medicine recommends using plant decoctions to rinse diaper rash on a baby's bottom.
There are a large number of folk remedies, which are based on medicinal herbs and even food. They effectively eliminate diaper rash on a baby’s bottom without harming him. But before using herbs, you need to make sure that your baby does not have an allergic reaction to it. Let's look at the most used ones:
- A decoction of the string. The herb brewed with boiling water is filtered and the decoction is added to the bathing water. You also need to wipe the damaged areas with a decoction of the string. The first result will appear the next day, and after 3-4 days significant improvements will be noticeable.
- Oak bark. Brewed bark at the rate of 4 tbsp. l. 1 liter of boiling water is added to the baby’s bathing water. After bathing, there is no need to rinse your baby; just pat dry with a towel.
- Chamomile. Chamomile decoction is also added when bathing. To prevent addiction to one herb, decoctions can be alternated.
- Apricot kernel oil. Excellent for dry damage.
Return to contents
Is it possible to completely restore intestinal function with surgery?
Obviously, with a successful combination of circumstances, which include a favorable form of the defect, the experience and skills of the surgeon, the equipment of the clinic, careful preparation for the operation and scrupulous postoperative care, the likelihood of a favorable result will be high. It should be taken into account that in order to achieve maximum results, the surgeon must solve the problem efficiently and on the first try. It has been proven that each subsequent reconstructive operation performed after a failed first one will have a less favorable prognosis. However, even with successful restoration of a number of intestinal functions after the first operation, important nerves and muscles responsible for the urge to empty the rectum and allow for retention of intestinal contents may be absent. Therefore, after the operation, they begin a rehabilitation program for intestinal functions, which includes elements of training and education that help children become neat.