Becker's nevus is an epidermal patch with hyperpigmentation and increased hair growth. The disease is more common in males. The first manifestations of the disease are usually observed at the age of 10–15 years. According to statistics, Becker's melanosis affects about 0.5% of men. Women suffer from this pathology much less frequently, since it is accompanied by minor anomalies in fetal development that occur under the influence of harmful factors.
Becker's disease is more common in males
Table of contents
- Etiology and pathogenesis
- Clinical manifestations
- Principles of treatment
Deep pigmentation is a congenital or acquired hypermelanosis, in which the bulk of excess pigment lies in the dermal layer of the skin.
In our company you can purchase the following equipment for removing deep pigmentation:
- M22 (Lumenis)
- Fraxel (Solta Medical)
Etiology and pathogenesis
Congenital dermal melanocytosis (Mongolian spot)
Hereditary hyperpigmentation caused by the active recruitment of melanocytes into the dermis as they migrate from the neural crest to the epidermis. The etiology of this disease is associated with a violation of the structure of G-proteins - these are GTPase proteins that act as second messengers in intracellular signaling cascades.
The prevalence of Mongolian spots varies among different ethnic groups. They occur most often in East African children with dark skin (up to 80%), somewhat less frequently in Latin American children (up to 46%), and extremely rarely in light-skinned Europeans (1–9%).
Histological examination of Mongolian spots reveals highly branched melanocytes, which are located in the deep reticular dermis and contain many pigmented melanosomes ( Fig. 1 ). Typically, melanocytes are oriented parallel to the epidermis.
Rice. 1. Histological changes in the Mongolian spot (Dermpedia)
https://www.dermpedia.org/dermpedia-textbook/mongolian-spot
Melanosis (nevus) of Becker
Its etiology and pathogenesis remain unknown to date. Androgens play a certain role, as evidenced by the presence of concomitant hypertrichosis and the predominance of this hypermelanosis in men. Thus, a study of 19,302 men aged 17–26 years found that the prevalence of Becker melanosis was 0.52%.
Microscopy reveals an increase in the amount of melanin in the basal layer of the epidermis. Melanosomes increase in keratinocytes, and giant melanosomes can be detected in both keratinocytes and melanocytes. The dermis contains melanophages—macrophages that have phagocytosed excess pigment ( Fig. 2 ).
Rice. 2. Histological changes in Becker's nevus (Parth P., et al. Sebaceus and Becker's nevus: Overview of their presentation, pathogenesis, associations, and treatment. Am J Clinic Dermatol 2015)
Lentigo
A widespread pigmentary disorder usually associated with chronic sun exposure of the skin. In the United States, lentigenic changes are observed in 90% of people with fair skin over the age of 60 years and in 20% of people under 35 years of age. The main cause of solar and senile lentigo is prolonged insolation; PUVA lentigo occurs after PUVA therapy (therapeutic effects on the skin of ultraviolet A radiation with preliminary intake of the photosensitizer psoralen); radiation lentigo - after large doses of ionizing radiation.
Solar lentigo is histologically characterized by elongation of the epidermal ridges, an increase in the number of melanocytes, which produce excess pigment, and the number of melanophages - macrophages that have absorbed the pigment and become dark in color. Atypical melanocytes are usually not detected in solar lentigo ( Fig. 3 ).
With PUVA lentigo, there is an increase in the number of hypertrophied melanocytes, often with signs of cellular atypia. Additionally, elongated epidermal ridges and increased pigmentation of cells in the basal layer of the epidermis can be seen. The same changes can be seen in lentigines after multiple visits to the solarium (tanning-bed lentigines).
Radiation lentigo is manifested by excessive deposition of melanin granules in basal keratinocytes, cellular or nuclear atypia, an increase in the number of melanocytes, and a decrease in the number of epidermal ridges.
Senile lentigo is characterized by proliferation of basal cells with the formation of cords containing excess melanin. An increase in the number of melanocytes in the area of the dermal-epidermal junction may also be detected. In general, melanocytes in senile lentigo have higher activity and longer processes than normal. By electron microscopy, large complexes of melanosomes are visible in keratinocytes.
Rice. 3. Histological changes in lentigo (Dermpedia)
https://www.dermpedia.org/dermpedia-textbook/lentigo-simplex
Melasma
Recurrent acquired dyschromia, caused by increased activity of epidermal-melanin units. Occurs in areas of the skin exposed to severe and/or regular sun exposure, more often in women of reproductive age.
Patients with melasma have an increase in the amount of melanin in the epidermis, dermis, or (most often) both of these layers of skin. Epidermal melanin is detected in keratinocytes of the basal and suprabasal region. The number of melanocytes in most cases does not increase, but the existing pigment cells are larger - they have pronounced processes and much higher activity than normal. Melanin is also detected in mecrophages of the superficial and middle dermis, which often collect around small dilated vessels ( Fig. 4 ).
Rice. 4. Histological changes in melasma (Nooshin B., et al. An overview on melasma. Pigmentary Disorders 2015; 2: 216)
Post-inflammatory hyperpigmentation
One of the common dermatological conditions that most often develops in people with dark phototypes (V-VI). Pathogenesis is associated with hyperproduction of sebum by the sebaceous glands and the presence of excess squalene on the skin (for example, with acne). Solar ultraviolet radiation generates singlet oxygen, which oxidizes squalene. The latter stimulates the production of prostaglandin E2, which triggers active melanogenesis.
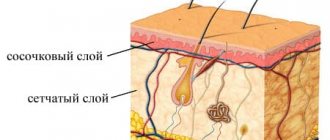
On microscopy, post-inflammatory hyperpigmentation can manifest as both epidermal and dermal increases in pigment ( Fig. 5 ). In the latter case, there is an increase in the number of melanophages in the papillary dermis. Dermal hyperpigmentation can last for many years or even last a lifetime.
Rice. 5. Histological changes in post-inflammatory hyperpigmentation secondary to systemic lupus erythematosus (Dr. Andrew Ryan, pathologist)
Histological changes in post-inflammatory hyperpigmentation
Forecast
In some patients, as they mature and grow, the size and intensity of the color of the giant nevus decreases somewhat. But the transformation of a benign giant nevus into a malignant melanoma occurs in 1.5–13% of patients (including in childhood), so patients should be monitored by an oncologist for life (even after removal of this pigmented formation). In addition, they should beware of excessive insolation, mechanical and chemical effects on the giant pigmented nevus.
Clinical manifestations
Congenital dermal melanosis (Mongolian spot)
The Mongolian spot is characterized by blue-gray macular pigmentation. A characteristic change in the color of the spot and the appearance of a bluish tint at different viewing angles is due to the Tyndall effect - the scattering of light as it passes through a heterogeneous medium.
Lesions can be single or multiple, occupying an area from a few square centimeters to affecting large areas of the body. Most often, the Mongolian spot is localized in the lumbosacral region, but can spread to the buttocks, back, shoulders, etc. ( Fig. 6 ) Generalized Mongolian spots have been reported, involving the entire anterior and posterior surface of the body, including the limbs.
Mongolian spots are often associated with cleft lip, spinal meningeal tumor, melanoma, and pigmentovascular phakomatosis (congenital hypermelanosis involving melanocytic and/or epidermal nevi).
Rice. 6. Congenital dermal melanosis - multiple Mongolian spots on the back (Danish national service on dermato-venereology)
Melanosis (nevus) of Becker
An early manifestation of Becker's nevus is an asymptomatic light or dark brown spot of uneven color and contour. It most often appears above the shoulder, on the upper chest or on the back. After several months or years, thick brown or black hair begins to grow in and around the nevus ( Fig. 7 ). The central area of melanosis may thicken with the development of acne (acne vulgaris).
Rice . 7. Becker's melanosis with dark hair (Danish national service on dermato-venereology)
Lentigo
Solar lentigo appears as flat or slightly concave round spots of varying diameters, light brown or dark brown in color. They usually appear in open areas - on the face, the backs of the arms and hands, and the upper half of the body ( Fig. 8 ). Immediately after its appearance, the size of solar lentigo is very small (less than 5 mm), but later the lesions become larger, darker and merge into large spots. They may contain areas of normal skin or be separated by fine wrinkles.
Lentigines after a solarium (tanning-bed lentigines) are similar to sunburn, but are detected in atypical places on the patient’s body, where a lot of sun usually does not reach - the inner surface of the arms and thighs, the armpit area, etc. The formations have a diameter of 2 to 5 mm, color brown or black. They appear suddenly after intense tanning, or after a long (1 year or more) regular visit to the solarium. The malignant potential of these lesions is not fully understood.
With PUVA lentigo, pigment spots are also similar to solar lentigo, but have irregular contours. After stopping phototherapy sessions, small lesions remain on the skin for up to 3–6 months, large lesions for up to 2 years.
Radiation lentigo includes additional signs of long-term radiation damage to the skin - subcutaneous fibrosis, keratosis, telangiectasia.
Rice . 8. Solar lentigo (Danish national service on dermato-venereology)
Melasma
It appears as a single lesion or multiple foci of dark brown or black hyperpigmentation, symmetrically located on the face and/or neck ( Fig. 9 ). According to localization, melasma can be centrofacial (forehead, cheeks, nose, upper lip and chin), malar (nose and cheeks) and mandibular (in the lower jaw area). In rare cases, melasma appears on the forearm and is associated with progesterone use.
Some areas of a patient's face may remain intact with melasma, and the cause of this is currently unknown. It is believed that this feature is associated with the density and activity of the sebaceous glands on the skin.
Rice . 9. Melasma (Danish national service on dermato-venereology)
Melasma
Post-inflammatory hyperpigmentation
The distribution of hypermelanotic lesions depends on the location of the original dermatosis or the site of injury. Their color varies from light brown to black - if the pigment is located in the dermis, the shade will be darker ( Fig. 10 ).
Rice. 10. Post-inflammatory hyperpigmentation on the leg (AboutKidsHealth)
https://assets.aboutkidshealth.ca/akhassets/PMD_post_inflammatory_hyperpigmentation_EN.jpg?RenditionID=10
What to do if a child scratches or tears off a mole?
In most cases, nevi are not a cause for concern. The appearance of moles in a child of any age is absolutely normal. They will gradually increase along with the growth of the child himself, and the location of the moles can be anywhere, including on the head, soles and even the genitals. Moles in children can easily be irregular in shape, have uneven borders, varied color patterns and large size, especially for congenital nevi.
It is also normal that moles will arouse your child's curiosity. If a child scratches or even picks off a mole, do not panic. This is only a reason to contact a dermatologist for dermatoscopy and further observation. So the answer to the question of what to do if your baby picks a mole is very simple: don’t worry and make an appointment with a specialist. ⠀
Parents need to be wary only in the following cases:
- rapid, sudden growth of formation in volume or diameter;
- the appearance of bleeding or a crust on the surface of the mole without previous injury;
- a rare type of mole;
- a large number of moles (>50) or cases of melanoma in the family;
- positive “ugly duckling” symptom (one formation is very different from other moles).
If you or your child just touched a mole, there is no need to worry.
Principles of treatment
Deep pigmentation does not respond well to external treatment methods, since the pigment lies quite deep in the skin - and it is extremely difficult to influence it from the outside. Whitening agents such as hydroquinone, tranexamic or azelaic acid can have a certain effect in some conditions (for example, melasma). There is evidence of the benefits of chemical peels, but you should be extremely careful not to cause even more pigmentation in the treated area.
Deep pigmentation is successfully treated with hardware methods - intense pulsed light (IPL) and lasers. The operating principle IPL therapy is based on selective photothermolysis - the absorption of light radiation energy by melanin with the subsequent destruction of unwanted pigment. For more precise exposure and prevention of heating of the surrounding skin, the IPL module of the M22 device from Lumenis uses a set of light filters. Each of these filters cuts off the wavelength range most suitable for a certain pigment depth and phototype.
If the pigment lies very deep, intense pulsed light may not be effective enough - in this case, non-ablative fractional photothermolysis is recommended Fraxel and M 22 ResurFX devices . Fraxel includes a 1550 nm erbium laser to work at the dermal level up to 1400 µm (1.4 mm) deep, as well as a 1927 nm thulium laser to work at the epidermal level up to 210 µm (0.21 mm). ResurFX uses one wavelength - 1565 nm, but this module can be combined in the M22 device with an IPL module and an Nd:YAG Q-Switched laser, so you can successfully treat any form of pigmentation.
Non-ablative fractional photothermolysis is based on the creation of microthermal treatment zones in the skin - tiny foci of thermal damage, between which there are intact (untouched) areas. This allows not only to effectively destroy unwanted pigment, but also accelerates subsequent skin restoration, because cells from intact areas migrate to microzones of damage. Non-ablative fractional photothermolysis is the method of choice in patients with skin phototypes IV–VI, who can undergo IPL therapy with restrictions.
Questions from our users:
- deep skin pigmentation on the hands
- deep skin pigmentation on the hands treatment
- deep skin pigmentation laser removal
- age-related deep skin pigmentation