April 28, 2021
Coin-shaped eczema (nummular eczema) is one of the types of chronic itchy dermatitis and microbial eczema, accounting for about 10% of the total number of dermatoses. A clear sign of the disease are large, round plaques with clear boundaries that rise above healthy skin. In children, coin-shaped eczema practically does not occur; among adults, it is approximately equally common, but most often occurs at the age of 30-50 years.
Why does coin-shaped eczema occur?
Doctors cannot yet clearly name the cause of coin-shaped eczema. What is known for sure is that the disease always has an infectious component. At the same time, such eczema is considered polyetiological, i.e. it can be caused by many different reasons. But regardless of this, infection always plays a major role in the development of dermatitis, which suppresses the immune system.
According to modern dermatologists, coin-shaped eczema is caused by a violation of the immune system: cellular (it is provided by leukocytes) and humoral (antibodies are the defenders - special proteins produced by cells). This is due to the fact that the body has a focus of chronic infection (otitis, tonsillitis, rhinitis), to which excessive sensitization occurs - increased sensitivity to the influence of irritants, causing allergies.
The risk of encountering coin-shaped eczema increases:
- in case of malfunction of the nervous system;
- changes in hormonal levels;
- excessive sweating;
- diabetes mellitus;
- frequent stressful situations;
- metabolic disorders;
- poor nutrition;
- chronic diseases of the ENT organs;
- oral infections.
To the list of factors, you can add medications that, against the background of a hereditary predisposition to dermatitis, reduce immunity and can cause coin-shaped eczema. Heredity is no less important in the development of the disease. If one of the parents has such a diagnosis, then the probability of its occurrence in the child is 40%, if both - then 60%.
Modern features of the clinic, diagnosis and treatment of patients with eczema
Eczema is an acute or chronic relapsing disease characterized by an inflammatory reaction formed under the influence of exogenous or endogenous factors, polymorphism of rash elements, and severe itching [1, 2]. The problem of eczema is currently becoming more and more urgent. In the structure of the incidence of chronic dermatoses, eczema accounts for up to 40% of all skin diseases. The incidence of eczema occurs in all age groups and often accompanies occupational diseases. According to the results of epidemiological studies, different types of eczema are among the most common diseases in the practice of a dermatovenerologist. The incidence among people of the working population is up to 10% [3]. Loss of temporary ability to work reaches 36% of all labor losses due to dermatoses. Among hospitalized patients, patients with eczema account for more than 30% [4]. The incidence of eczema is higher among women than among men. In recent years, eczema has tended to become more severe with frequent relapses, significant spread of the process on the skin and resistance to treatment [5].
Eczema develops as a result of the complex influence of etiological and pathogenetic factors, including endocrine-metabolic, infectious-allergic, vegetative-vascular and hereditary [6]. Great importance in the formation of eczema is attached to the immunogenetic characteristics of the body - association with the HLA-B22HLA-Cw1 antigen of the body [2]. Genetic predisposition determines disruption of immune regulation, function of the nervous and endocrine systems. In eczema, polygenic multifactorial inheritance occurs with pronounced expressivity and penetrance of genes. If one of the parents (mainly the mother) is ill, the chance of developing eczema in a child is 40%, and if both parents are ill, up to 60% [6]. The pathology of the gastrointestinal tract and hepatobiliary system is of important pathogenetic significance. Failure of the intestinal barrier, most typical for children, leads to the absorption of undigested protein into the blood [2]. Allergic reactivity also plays a major role in the development of eczema.
According to modern concepts, the main role in the development of eczema is played by T-lymphocytes, which carry specific antigen receptors on their surface and secrete a number of pro-inflammatory cytokines that cause the development of tissue inflammatory reactions. Exogenous influences are extremely diverse. They cause eczematous skin changes through the mechanism of delayed-type hypersensitivity, caused by contact with chemical, biological, drugs and antigenic microbial determinants in foci of chronic infection [6, 7].
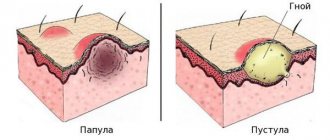
Clinical signs of eczema may include itching, redness and flaking of the skin, and the presence of grouped papulovesicles [2]. During the eczematous process, the following stages can be distinguished: erythematous, papular, vesicular, weeping stage, cortical stage, peeling stage [1]. Depending on the characteristics of the clinical picture, the following forms of eczema are distinguished [2]:
- true eczema: idiopathic, dyshidrotic, pruriginous, horny (tilotic);
- microbial eczema: numular, paratraumatic, mycotic, intertriginous, varicose, sycosiform, eczema of the nipples and the areola of the young gland of women;
- seborrheic eczema;
- childhood eczema;
- eczema occupational.
True eczema
In the acute stage, true eczema is manifested by the appearance of vesicles, erythema, point erosions with weeping, serous crusts, excoriations, but there may be papules and pustules. The boundaries of the lesions are unclear. The process is symmetrical; the face and limbs are most often affected, with alternation of healthy and affected skin. The process can also spread to other areas of the skin, including erythroderma. After the transition to the chronic stage, hyperemia becomes stagnant, areas of lichenification and cracks appear. Often the process can be complicated by pyogenic infection; purulent crusts and pustules appear [8].
Monetoid (numular) eczema
Numular eczema is predominantly a disease of adults. Males are affected more often than females. The peak incidence in both sexes occurs between 50 and 65 years of age. The second peak in women occurs between the ages of 15 and 25 years. In newborns and children, nummular eczema is a rare disease. In children it starts at age five. The pathogenesis of nummular eczema is still unknown. Most patients have no personal or family history of atopy, but nummular plaques may be present in tropical eczema. Many factors are considered as the cause of the disease. Elderly patients experience decreased skin hydration. In 68% of patients, foci of infection were identified, including in the dental area and respiratory tract. Environmental allergens, such as house dust mites, also play a role in the occurrence of nummular eczema. Clinically, well-circumscribed, coin-shaped plaques of confluent papules and papulovesicles are visualized. Characteristic signs are pinpoint weeping and the formation of crusts. However, crusts may cover the entire surface of the plaque. The size of the plaques ranges from 1 to 3 cm in diameter. The surrounding skin is normal in most cases, but may be xerotic. The intensity of itching varies from minimal to severe. Resolution of elements in the center may be observed, which is noted in ring-shaped forms of the disease. Chronic plaques are dry, scaly and lichenified. The classic location of lesions is the extensor parts of the limbs. In women, the upper extremities, including the dorsal surface of the hands, are more often affected than the lower extremities.
Microbial eczema
Microbial eczema is a polyetiological disease. The role of the skin barrier in the pathogenesis of microbial eczema is important. Violation of the integrity of the skin during its resorption due to itching forms an entrance gate for infection. Exudation that accompanies eczema promotes the concentration of proteins on the surface of the skin and creates favorable conditions for the proliferation of secondary infections. The state of the skin microbiota in patients with microbial eczema is of great importance. In scrapings of the affected epidermis in patients with microbial eczema, Staphylococcus aureus, Staphylococcus haemolyticus, non-lipophilic yeast fungi, mainly of the genus Candida spp. The leading pathogens of microbial eczema are infectious allergens - bacterial, viral, fungal protozoans and others. The disease can also be provoked by exogenous stimuli - physical, mechanical and biological. The immunoallergic theory is clearly confirmed by the empirically identified stages of the course of microbial eczema. Initially, the disease develops in the form of eczematization at the site of non-allergic pyodermatitis, and then through localized forms it is transformed into a generalized process. Foci of microbial eczema often occur in areas of long-persistent pyoderma and around purulent wounds. Microbial eczema is a complication of dermatophytosis of large folds and feet, superficial candidiasis of the skin. Initially, sensitization may be monovalent in nature, but over time it becomes polyvalent. In the pathogenesis of microbial eczema, a decisive role is played by bacterial sensitization by Staphylococcus aureus and Staphylococcus haemolyticus. Patients with microbial eczema develop an immunologically caused latent syndrome of endogenous intoxication. An increase in the concentration of circulating immune complexes and the value of the leukocyte index of intoxication are directly proportional to the intensity of immunopathological processes [9, 10]. Microbial eczema mainly manifests itself as asymmetrical lesions. The lesions are round or irregular in shape, have clear boundaries, and are limited by a border of exfoliating epidermis. The central part of the lesions is covered with purulent and serous crusts; after their removal, a weeping surface is revealed, having the appearance of “wells”. The rash is accompanied by intense itching [1].
Seborrheic eczema
Seborrheic eczema begins on the scalp. The lesions spread to the behind-the-ear areas, neck, upper chest, interscapular area, flexor surface of the limbs; Like seborrheic dermatitis, seborrheic eczema is localized in areas of the skin with a large number of sebaceous glands and does not have clear boundaries. Within the lesions, the skin is hyperemic, swollen, small yellowish-pink papules, fatty yellowish scales and crusts are visible on its surface [1].
Varicose eczema
Varicose eczema is associated with the presence of varicose veins in the patient. The lesion is localized on the skin of the lower extremities, mainly in close proximity to varicose ulcers, mainly in the lower third of the leg. Skin maceration, various injuries, and irrational treatment of varicose ulcers play a role in the development of the disease. The disease is accompanied by itching. Differentiate with erysipelas, pretibial myxedema [3, 11–13].
Sycozyform eczema
Sycosiform eczema develops against the background of vulgar sycosis, the pathological process spreads beyond the area of hair growth. As a rule, the skin process is localized on the chin, pubis, upper lip, and axillary region. Clinically, itching and weeping, serous wells are noted, and with the passage of time, areas of skin lichenification appear [2].
Childhood eczema
Childhood eczema manifests itself with clinical signs of true, microbial and seborrheic eczema. The first manifestations appear at the age of 3–6 months. Exudation processes predominate on the skin. The affected areas are symmetrical, brightly hyperemic, edematous, pronounced weeping, layering of crusts. Milk crusts appear. Erythematous lesions have a shiny surface and are hot to the touch. The affected areas are localized on the cheeks, forehead, ears, scalp, extensor surfaces of the limbs, and buttocks. The nasolabial triangle remains untouched. Patients are bothered by itching and insomnia. At the age of 2–3 weeks of life, against the background of reduced nutrition, a characteristic clinical picture of the disease may develop. It often transforms into atopic dermatitis [2, 11, 14, 15].
Eczema of the nipples
Nipple eczema is a consequence of trauma to the nipples while breastfeeding, but in some cases the etiology cannot be determined. It is characterized by slight erythema, mild infiltration, weeping and the presence of serous-hemorrhagic crusts, the appearance of pustules and cracks is possible. Usually the pathological process is bilateral in nature and is not accompanied by nipple hardening [2].
Occupational eczema
Occupational eczema develops under the influence of industrial allergens. Occupational allergens include metal alloys, mercury compounds, penicillin and semi-synthetic antibiotics, epoxy resins, and synthetic adhesives. With occupational eczema, a delayed-type hypersensitivity reaction develops. The clinical picture has all the signs of ordinary eczema. Occupational eczema develops mainly in exposed areas of the skin, in areas of contact with an irritant. When the etiological factor disappears, the disease quickly resolves [11, 16].
Paratraumatic eczema
Paratraumatic eczema develops in the area of postoperative scars, in places of improper application of plaster casts, in places of osteosynthesis. Clinically, acute inflammatory erythema occurs, papules or pustules appear, with further formation of crusts. Deposition of hemosiderin in affected tissues is possible [2].
Diagnosis is based on the history and clinical picture of the disease. Laboratory tests are carried out: biochemical blood test with determination of ALT, AST, triglycerides, total protein, creatinine, total bilirubin, glucose; general blood analysis; clinical urine analysis; determination of the level of total IgE in serum using ELISA; skin tests; determination of antibodies to antigens of Giardia, Ascaris, Toxocara and others; histological examination of skin biopsies is carried out according to indications for the purpose of differential diagnosis. The diagnosis of occupational eczema is confirmed by skin testing with suspected occupational irritants. Diagnosis, examination and treatment of a patient with eczema depend on recognizing eczematous changes on the skin, determining the severity of the process and characterizing the rashes in order to classify the forms of eczema the patient has. According to indications, consultations with other specialists are prescribed - an endocrinologist, an allergist, a therapist, a gastroenterologist [2].
In case of true eczema, differential diagnosis is carried out with pyoderma, allergic contact dermatitis, atopic dermatitis, and toxicoderma. Differential diagnosis of coin-shaped eczema is carried out with plaque parapsoriasis, pityriasis rosea, and seborrheic eczema. Seborrheic eczema is differentiated from Darier's collicular dyskeratosis and Devergie's disease. Microbial eczema is differentiated from streptoderma, allergic contact dermatitis, and leishmaniasis. Differential diagnosis of sycosiform eczema is carried out with vulgar sycosis. Dyhydratic eczema must be distinguished from pustular bacteridosis, dermatomycosis, palmoplantar psoriasis, pustular psoriasis of the palms, and chronic acrodermatitis of Allopeau [6, 10, 14, 15, 17, 18].
When treating the acute stage of eczema, first generation antihistamines are used. Glucocorticosteroid drugs are used in the presence of severe inflammation. For severe skin itching, a tranquilizer with an antihistamine effect is prescribed. If there is severe exudation, detoxification therapy is prescribed. In the presence of microbial eczema, secondary infection, lymphangitis, lymphadenitis, and fever, antibacterial drugs are used. For tylotic eczema in cases of severe infiltration, hyperkeratosis and/or torpidity, it is recommended to prescribe retinoids to the therapy.
Apply lotions with 1% tannin solution, 2% boric acid solution, 0.25% silver nitrate solution, baths with 0.01–0.1% potassium permanganate solution, Tsindol solution 1–2 times a day for 4–7 days . Antiseptic external preparations (brilliant green alcohol solution 1% or Fukortsin alcohol solution) are prescribed externally to the area of the rash 2-3 times a day for 5-14 days. Glucocorticosteroid drugs 1-2 times a day externally for 7-20 days. As acute inflammatory phenomena subside, pastes containing 2–3% ichthammol, naphthalan oil, 0.5–1% sulfur, 2–5% boron zinconaphthalan paste, and 2–5% tar-naphthalan paste are used. Physiotherapeutic treatment includes narrow-band mid-wave ultraviolet therapy with a wavelength of 311 nm, 4-5 times a week, for a course of 25 to 30 procedures. When following a diet, eggs, citrus fruits, poultry, fatty fish, meat broths, whole milk, nuts, carbonated drinks, red wines, and seafood are excluded from the diet of patients with eczema [2].
Thus, eczema is one of the most common diseases resulting from the action of both external and internal factors. The complexity of the pathogenesis of eczema requires an integrated approach to its treatment, taking into account the severity of the process, the form of the disease, the state of internal organs and systems, which requires an individual approach to the management and treatment of patients.
Literature
- Vladimirov V.V., Zudin B.I. Skin and venereal diseases. Atlas. 2nd edition. M.: Medicine. 2012. 288 p.
- Federal clinical guidelines. Dermatovenereology 2015: Skin diseases. Sexually transmitted infections. 5th ed., revised. and additional M.: Business Express, 2016. 768 p.
- Makhulaeva A. M. Results of complex treatment of patients with varicose ecema of the leg associated with mycotic infection // Almanac of Clinical Medicine. 2010. pp. 219–224.
- Nikonova I.V. State of skin biocenosis in microbial eczema // Practical medicine. 2011. pp. 80–83
- Kurbanova A. A., Kisina V. I., Blatun L. A. Rational pharmacotherapy of skin diseases and sexually transmitted infections. A guide for practicing doctors. M., 2012. pp. 406–407.
- Dermatovenerology. National leadership / Ed. Yu. S. Butova, Yu. K. Skripkina, O. L. Ivanova. M.: GEOTAR-Media, 2022. 896 p.
- Yusupova LA Level sl-selectin in blood serum of patients with schizophrenia comorbidity pyoderma // European journal of natural history. 2013. No. 3. pp. 19–20.
- Wolfe K., Johnson R., Surmond D. Dermatology according to Thomas Fitzpatrick. Atlas-directory. 2007. 1312 p.
- Sokolova T.V., Malyarchuk A.P., Safonova L.A. Strategy for choosing external therapy for microbial eczema // Clinical dermatology and venereology. 2022, 3, 46–51.
- Yusupova L. A. Prevalence of athlete's foot in patients with mental disorders. In the book: Advances in medical mycology. Sat. scientific tr. M., 2003. T. II. pp. 201–202.
- Dagilova A. A. General approaches to the treatment of eczema in the practice of an internist // Treating Doctor. 2012, no. 8, p. 15–17.
- Yusupova L.A. Current state of the problem of skin angiitis // Attending Physician. 2013, no. 5, p. 38–43.
- Lehucher-Michel MP Dyshidi eczema and occupation: A descriptive study // Contact Derm. 2000. 43. R. 200.
- Yusupova L. A. Diagnosis and complex therapy of atopic dermatitis in patients with mental disorders // Bulletin of postgraduate medical education. 2003. No. 2. pp. 11–14.
- Warshaw EM Therapeutic opt for chronic hand dermatitis // Dern. Ther. 2004. 17. R. 240.
- Yusupova L. A. Prevalence of chronic dermatoses in patients with mental disorders // Bulletin of postgraduate medical education. 2003. No. 3–4. pp. 46–48.
- Swartling S. Treatment of dyshidrotic hand dermatitis with intradermal botulinum toxin // Am A Dermatol. 2002. 47. R. 667.
- Holden K. Eczema and contact dermatitis. MEDpress-inform, 2009. 112 p.
L. A. Yusupova*, 1, Doctor of Medical Sciences, Professor E. I. Yunusova*, Candidate of Medical Sciences Z. Sh. Garayeva*, Candidate of Medical Sciences G. I. Mavlyutova*, Candidate of Medical Sciences E. V. Bildyuk* * A. N. Shakirova *
*GBOU DPO KSMA Ministry of Health of the Russian Federation, Kazan **GAUZ RKKVD, Kazan
1 Contact information
Modern features of the clinic, diagnosis and treatment of patients with eczema L. A. Yusupova, E. I. Yunusova, Z. Sh. Garayeva, G. I. Mavlyutova, E. V. Bildyuk, A. N. Shakirova For citation: Attending physician no. 6/2018; Page numbers in the issue: 85-87 Tags: dermatosis, inflammation, etiology, risk factors
How does coin-shaped eczema manifest?
The peculiarity of coin-shaped eczema is that the skin with this disease is in constant readiness to interact with the irritant. Moreover, reactions appear gradually: first, the skin reacts to one thing, and then to many different antigens.
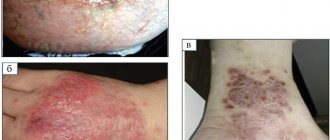
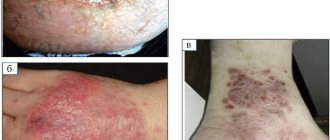
A characteristic symptom of coin-shaped eczema is oval-shaped spots with a diameter of up to 3 cm. They have clear outlines and rise above the surrounding healthy skin. The spots most often occur on the skin of the extremities, but can spread to the upper back, shoulders and buttocks.
The rash causes severe and sometimes unbearable itching, interfering with normal sleep. Because of this, a person scratches them, which leads to the appearance of crusts. Along the borders of the spots there are vesicles that open up and form erosions. When the inflammation subsides a little, the skin dries out and cracks form on it. With exacerbation, spots appear in the same areas.
Many people are interested in the contagiousness of coin-shaped eczema. Like other types of dermatitis, it is absolutely not contagious and cannot be transmitted to other people even through close contact. Therefore, a person with such a diagnosis cannot infect anyone, and being with him is completely safe.
Treatment with folk remedies
Alternative medicine can be an addition to primary therapy, but you should not rely on it alone for treatment. Even the most effective recipes will not provide the same effect as medications.
| Recipe | Composition and method of application |
| Cabbage compress | Wash the cabbage leaves, pour over boiling water, and chop until smooth. Add 1 egg white, mix. Apply the prepared mixture to the affected area for 30 minutes. Repeat several times a day. |
| Potato compress | Wash the potato tubers without peeling and chop them. Add honey and stir. Apply to inflamed areas. The recipe is contraindicated if you are allergic to bee products. |
| Sea buckthorn oil | Sea buckthorn oil, purchased at a pharmacy, relieves itching well. After treating the skin, apply a cotton pad soaked in oil to the affected areas. It moisturizes well and starts regenerative processes. |
| Decoction of elderberry and St. John's wort | 100 g of dry raw materials (50 g of St. John's wort and elderberry) pour 1 liter of water. Bring to a boil over low heat. Remove, cool, strain. Rinse the inflamed areas with the broth 2-3 times a day. |
How is coin-shaped eczema diagnosed?
A dermatologist may suspect coin-shaped eczema based on external signs. To confirm, standard tests are prescribed, including a general analysis of urine and blood, and a biochemical blood test. The patient may need to consult a neurologist, gastroenterologist, allergist and endocrinologist.
Coin-shaped eczema must be distinguished from other types of dermatitis, psoriasis, scabies and dermatomycosis. For this purpose, an enzyme immunoassay test of blood for antibodies is performed. To identify an infection, a microbiological examination of a smear from the site of inflammation is carried out. It also helps determine antibiotic sensitivity and prescribe the correct treatment.
How to cure coin-shaped eczema
Treatment of coin-shaped eczema is complex. It is necessary to take measures against the underlying disease, which is associated with a source of chronic infection, to normalize the functioning of the digestive, endocrine and nervous systems. Antibiotics help with coin-shaped eczema, but often do not lead to remission, which is what needs to be achieved with such a disease.
Antibacterial drugs are often resorted to if a secondary infection has occurred. In other cases, the basis of treatment is:
- sedatives, tranquilizers, antidepressants, antipsychotics, herbal teas - to relieve stress;
- desensitizing drugs - to eliminate allergies;
- enzymes - to improve digestion.
For external treatment of eczema, hormonal ointments are used, which give quick results. But before prescribing them, they resort to non-hormonal agents, which include zinc-based ointments and creams. For itching, topical steroids show good results. Physiotherapy procedures have a beneficial effect on the skin: ultraphonophoresis, acupuncture, UHF therapy, ozone therapy, therapeutic mud, paraffin applications.
It is equally important to follow a diet that excludes potential allergens: citrus fruits, marinades and pickles, fried and smoked foods, red fruits, seafood, nuts, honey, chocolate. The basis of the diet should include cereals, herbs, vegetables, and lactic acid drinks.
Treatment of coin-shaped eczema in children
A child is diagnosed with coin-shaped eczema by a dermatologist upon examination. For a detailed study of pathology, smears and scrapings are prescribed. Therapy in this case should be comprehensive.
Treatment should be carried out under the constant supervision of a doctor. Self-medication is strictly prohibited. This can harm the child and worsen the course of the disease.
| Group of drugs | Action/Name |
| Glucocorticosteroids | The local effect of these drugs is aimed at reducing itching and inflammation of the skin. Regenerative processes are launched. Hormonal drugs are prescribed only by a doctor; treatment has a certain time frame and is carried out under the supervision of a doctor. Prescribe hydrocortisone and prednisolone ointments |
| Corticoids | Preparations for topical use have many contraindications. Do not use on your own. A short period is suitable for treatment. Flucinar and Lokoid are prescribed. |
| Antibacterial | They have pronounced antifungal and antibacterial properties. They are prescribed when diagnosing microbial infection. Levomekol, Triderm, Clotrimazole are prescribed. |
| Solutions for skin disinfection | The skin should be treated with Fukortsin, a solution of manganese, and silver nitrate. |
| Preparations for recovery and wound healing | Regular use of Zinc ointment and Ichthyol is prescribed to accelerate wound healing. Doctors change medications periodically. So the body does not get used to them. |
Seek help from a dermatologist
It is important to confirm the diagnosis before prescribing either treatment or diet.
If you find suspicious rashes on your skin, be sure to consult a dermatologist. The effectiveness of treatment directly depends on the correctness of the diagnosis. Therefore, it is important not to delay or self-medicate. We invite you to a consultation at the PsorMak Institute for Healthy Skin. We have extensive experience in successfully treating various types of dermatitis, and we guarantee the achievement of long-term remission. April 28, 2021
Author of the article: dermatologist Mak Vladimir Fedorovich