Kluban Olesya Anatolevna
Neonatologist
April 29, 2017
Toxic erythema of newborns is a problem that 40 to 70% of mothers face on the 2nd-3rd day of a baby’s life. “Terrible pimples” are usually very scary for new mothers, and the diagnosis “Erythema toxicum” sounds so scary that some parents find themselves on the verge of panic.
But should we be afraid? Olesya Anatolyevna Kluban , a neonatologist at the ISIDA clinic, answers this question
Erythema toxicum, despite its scary name, is a benign non-infectious process that occurs during the adaptation period of newborns. It appears, as a rule, 48-72 hours after the birth of the baby, sometimes (rarely) immediately after birth and even less often - on the 10-14th day of life. This problem occurs equally among all races and both sexes and is more common in babies born at term weighing more than 2500 g.
Erythema toxicum: what is it?
Panic aside. Erythema toxicum is not at all toxic, although the name suggests that it is something dangerous and extremely contagious. Rashes on the body of a newborn are not caused by infections, pathogenic bacteria, or viruses.
As doctors say, this is a kind of physiological reaction of the baby’s body to changes in environmental conditions. This is how the child’s skin “adapts” to a completely new external world, which is still hostile.
Erythema toxicum is a reddish rash that usually appears 48-72 hours after the baby is born. Cases have been identified where small pimples on the skin appeared much later - after 10-20 days. Redness first affects the baby's face and torso, and then moves to the child's arms and legs. The mucous membranes, palms and soles remain clean.
Why does toxic erythema occur?
The causes of the rash are unknown. But doctors agree that toxic erythema appears due to the release of a large number of “allergy mediators” in the child’s body. This is a natural physiological process that occurs in the baby’s body in the first days and weeks of his life.
But there can be quite a lot of external factors that sometimes cause such a strong reaction in a baby, which is not similar to a “normal” allergy. Among them:
- activation of the newborn’s immune system;
- adaptation of the baby to the external temperature;
- inflammatory response of the skin to the “colonization” of normal bacterial flora from the environment;
- a skin reaction caused by lymphocytes transmitted by the mother before or during childbirth.
Also, the causes of the appearance of toxic erythema are associated with heredity, the mother's taking a number of medications and severe toxicosis, developed fetal hypoxia and intrauterine infection, and late onset of breastfeeding.
Scientists do not have an exact answer whether erythema toxicum appears more often in boys or girls. According to experts, the cause of the rash has nothing to do with gender. But according to the observations of scientists, an allergic reaction most often appears in full-term infants weighing more than 2500 kg.
Who is at risk?
The child is sleeping
In addition to babies, whose bodies are affected by the factors listed above, newborns who receive their mother’s breast milk are most often susceptible to the development of toxic erythema, oddly enough. This is due to the fact that a woman can eat prohibited foods, eat a lot of sugar, drink coffee, smoke, and drink alcohol.
All toxic substances and potential allergens enter the baby's body through breast milk, increasing the risk of developing toxic erythema and other pathological skin conditions. In babies who are bottle-fed and receive formula, erythema occurs much less frequently.
What do the rashes look like?
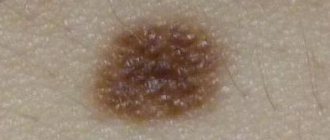
Rashes with toxic erythema look like small red spots from 0.1 to 2 cm in diameter. Usually accompanied by slight swelling. In general, in some ways they visually resemble flea or mosquito bites, as well as urticaria rashes. There can be many such spots - they cover literally the entire body of the child, merging with each other. It is precisely these physiological processes that frighten parents to the point of panic. But more often there are cases when redness does not cover the skin so “thickly”, but only isolated pimples are observed.
Inside the pimples, papules with whitish or yellowish pus may be observed. When you press on the affected areas of the skin, the redness fades a little.
Symptoms of toxic erythema
The appearance of red rashes is the main sign of toxic erythema. If the localization of acne is small, then the “allergy” is almost asymptomatic - nothing bothers the child.
But when redness spreads throughout the body, a number of unpleasant symptoms may appear - itching and flaking of the skin. It is natural for a newborn to become restless.
Physiological erythema does not cause symptoms such as high fever and indigestion. Therefore, if the rash is accompanied by other warning signs, it is better to consult a doctor. Most likely, the reason for the child’s poor health lies in another disease that requires examination by a specialist.
Causes
Before starting treatment for erythema in children, this disease should be accurately diagnosed and the causative agent identified. The thing is that this anomaly is often confused with other skin diseases - rubella, urticaria, dermatitis, etc. But this pathology requires certain therapy, so a correct diagnosis is extremely important.
The main cause of erythema in children, or rather redness of the skin, is dilation of the capillaries. But this is achieved by other factors that affect the child’s body both externally and internally. Due to the structural features of the dermis, this disease is not uncommon in children. The thing is that their blood vessels are located quite close to the surface, to the epidermis itself. And any provoking factor causes rapid expansion of small vessels. This is what leads to redness of the skin.
A large number of erythemas have completely normal, natural and safe causes. Redness on the skin in children may appear as a reaction to touch, including massage. At elevated air temperatures (in a bathhouse or sauna), capillaries can also respond - expand. Erythema appears in a child during active games or sports. The explanation is quite simple - the blood supply becomes more intense, and under blood pressure the capillaries become larger.
But the pathological causes of this disease are determined by:
- infectious diseases that the child had or has;
- chemical burns;
- thermal burns;
- allergic reactions;
- post-traumatic changes that are observed in the skin;
- diseases occurring against the background of elevated body temperature.
When should you see a doctor?
At the first symptoms of erythema in children, you should contact a highly specialized physician. Allergists treat such pathologies. They carry out an external examination, give directions for certain tests, and make a conclusion. Based on it, the diagnosis is either confirmed or refuted.
If you are looking for an experienced specialist, we recommend contacting JSC “Medicine” (clinic of academician Roitberg), located in the central district of Moscow at the address: 2nd Tverskoy-Yamskaya lane 10. Our clinic is located near the Mayakovskaya, Belorusskaya, Novoslobodskaya metro stations , Tverskaya, Chekhovskaya.
But what symptoms indicate erythema in children? Let's take a closer look.
What can erythema toxicum be confused with?
A red rash on a baby’s skin, no matter what the reason for it, is scary. It is unlikely that parents, without medical degrees, will be able to distinguish toxic erythema, which, in general, is completely harmless, from other dermatological diseases. You need to consult a specialist to rule out more dangerous skin diseases.
Toxic erythema may visually resemble urticaria, food allergies, or so-called milia - small white pimples on the face, the appearance of which is associated with the “transfer” of maternal hormones to the child. It is better to leave aside “grandmother’s recipes” for treating redness in children. Perhaps herbal baths will not make things worse - they will relieve the itching, soothing the newborn’s skin. But if pimples on the face and body are caused by food allergies, a completely different approach is needed - a review of the diet plan for mother and child. Baths and lotions will not solve the problem.
If the rash does not go away, consultation with a doctor is required.
How do doctors make a diagnosis?
The doctor usually makes the diagnosis based on a visual inspection of the red spots on the baby's skin. There are no difficulties in establishing the causes of the rash, since it appears in the first days of a child’s life. No tests will be required.
The following clinical forms of toxic erythema are distinguished:
- Localized. Single small red spots - usually only on the face, chest or around the joints. The newborn practically does not feel any discomfort and behaves calmly.
- Common. Red spots increase in size, spreading throughout the body and limbs. The rash may itch and peel, causing the newborn to become restless or, conversely, lethargic.
- Generalized. The pimples seem to merge into one red spot, their edges are difficult to distinguish. Ulcers form. The newborn becomes irritable because he is bothered by severe itching. In very rare cases, a rise in temperature may occur.
And according to its course, toxic erythema can be:
- Spicy. The rash appears on the first or second day after birth and disappears after 5-7 days. As a rule, in this case, the redness is localized.
- Lingering. Acne appears on the 1st-4th birthday, and disappears only after 2-3 weeks. It is possible for the rash to spread throughout the body. Typically, a prolonged course of erythema is observed if the newborn is not full-term.
When red spots do not go away within 3-4 weeks, the pediatrician will definitely recommend an examination by a dermatologist. And the specialist will already prescribe a histological examination of samples taken from flat spots, papules and pustules. Perhaps it is an allergy that manifests itself as severe redness.
Coronavirus in newborns (0 to 4 weeks) children
To date, there has been no evidence of intrauterine infection caused by mother-to-child transmission. All cases of coronavirus infection are considered acquired after the birth of the baby. As the incidence rate increases, the number of newborns infected by mothers with coronavirus infection has increased. Worldwide, only 5% of all recorded cases of COVID-19 occur in children under one year of age. Most often, infants experience an asymptomatic or mild course of the disease, which may be accompanied by a slight rise in body temperature.
Medical practice describes such symptoms of coronavirus in children in the first weeks of life as “groaning” breathing, increased work of the respiratory muscles, apnea, cough and tachycardia. Sometimes weak sucking, lethargy, regurgitation, diarrhea, and bloating are observed. Cases of covid pneumonia are extremely rare. Most often, a severe form of coronavirus occurs in children with congenital malformations. The risk of complications increases in the case of: prematurity, birth injuries, pulmonary dysplasia and tumors.
Treat or leave as is?
As doctors say, in most cases, physiological erythema disappears on its own without additional treatment. The child, in general, feels well. The rash will not harm him, will not infect other family members and will not be inherited. Just a week and your baby's skin will become clear.
But there have also been cases where the rash reappeared - in the first 6 weeks of the child’s life. If this happens, there is no need to worry - usually the process is much easier and does not occur again.
Despite the fact that no specific treatment is needed for erythema toxicum, doctors insist on the importance of maintaining baby skin hygiene. This will help eliminate the risks of complications of an allergic reaction in the form of severe itching and irritation, infection of inflamed pimples.
The rules are as follows:
- Do not rub areas with redness vigorously with a towel after a bath.
- Avoid overheating and hypothermia of the baby.
- Dress the newborn in clothes made from soft natural fabrics.
- Avoid tight swaddling.
- Give your child air baths more often.
- Change contaminated clothing promptly.
- Temporarily do not use special children's cosmetics, even if they are completely natural.
- Do not “coat” the child with ointments from the pharmacy or oil unless the doctor recommends it.
The skin of a baby is very delicate. And it is important that it is clean until the physiological redness has passed. Carmen Lee Wong, a pediatric dermatologist at the Children's Hospital of Eastern Ontario in Ottawa, recommends bathing your baby daily. But not for long - 2-4 minutes will be enough. According to the specialist, this will help the rash heal faster and help prevent it from spreading across the skin. Water will wash away saliva and pathogenic microflora, which often lead to the appearance of ulcers. When taking baths, you do not need to use cosmetics; just warm water will be enough.
Generalized toxic erythema is more complex. Due to the fact that the physiological rash is also accompanied by severe itching, which can be quite difficult for the child to tolerate, the doctor usually gives the following prescriptions:
- drinking plenty of water;
- antihistamines for oral administration;
- antiallergic ointments.
SKIN DISEASES IN CHILDREN IN THE FIRST YEAR OF LIFE: DIAGNOSIS ISSUES
Management of newborns and infants suffering from skin diseases requires accurate decisions and prompt actions from the dermatovekerologist, the effectiveness of which largely depends on correct and timely diagnosis. Pediatric dermatovenerology has now turned out to be not only an extremely responsible, but also the most difficult area for dermatovenerologists. Despite the fact that doctors of various specialties take part in the treatment of children with skin pathologies, it is not possible to achieve satisfactory results in terms of reducing the level of the disease and increasing the effectiveness of treatment and preventive care. The number of diagnostic errors is especially high. Pediatric dermatology is closely related to the prevention of hereditary pathology, since the birth of a sick child prompts relatives to consult a doctor to determine the genetic prognosis. Increasing the level of professional nosological diagnostics is the initial and necessary condition for the development of therapeutic, preventive and medical genetic care. Brief reviews are offered on the issues of diagnosis, treatment, prevention and rehabilitation of children suffering from skin and venereal diseases.
To cure neonates and babies who suffer from skin diseases requires that dermatovenerologist should take accurate decisions and make prompt actions whose effectiveness largely depends on correct and timely diagnosis. Pediatric dermatovenereology has proven to be not only a highly crucial but the most challenging area for dermatovenereologysts. Despite the fact that physicians of various disciplines participate in the treatment of infants with skin abnormalities, there are no saticfactory results in reducing incidence rates and enhancing therapeutical and preventive care. There are a great deal of diagnostic errors. Pediatric dermatovenereology is closely associated with the prevention of hereditary pathology as the birth of an ill baby makes his relatives to visit a doctor to determine a genetic prognosis. To enhance the level of professional nosological diagnosis is a primary and essential condition for the development of therapeutical, prophylactic, and medical and genetic care. Brief reviews on 1) diagnosis, 2) treatment, prevention, rehabilitation of infants, with skin and venereal diseases are proposed.
Department of Dermatovenereology (Head: Doctor of Medical Sciences, Prof. K. N. Suvorova) of the Russian Medical Academy of Postgraduate Education. Prof. KN Suvorova, MD, Head of the Department of Dermatovenerology, Russian Medical Academy of Postgraduate Training
Introduction
In children of the first year of life, various skin lesions are detected more often than in other age groups. The pathology of the skin during this period is distinguished by the pronounced specificity of the nosological profile and the unusualness of the clinical manifestations of dermatoses, which are also known in adults, but manifest differently. A dermatovenerologist should know about special skin conditions in newborns, specific approaches to the treatment of dermatoses, and the characteristics of an infant’s body that determine its response to medications or contribute to the severity and chronicity of dermatoses and the development of complications typical for this age. In the first months of life, suddenly severe and acute dermatoses may occur, when an accurate diagnosis and urgent assistance are urgently needed, which can only be provided through the joint efforts of pediatricians and dermatologists. Secondary skin lesions may occur with congenital metabolic defects and other multiple organ syndromes with onset in infancy; a dermatologist, having an adequate understanding of such diseases, must promptly refer the child to a pediatrician and other specialist in accordance with his diagnostic assumptions. On the other hand, often the most common skin lesions are first discovered by a pediatrician who constantly monitors the child. In such cases, he should be able to suspect a skin disease and refer the child to a dermatologist. The task of a pediatrician is to identify and treat internal diseases that contribute to the exacerbation or torpid course of dermatosis, and a dermatovenerologist is obliged to correctly diagnose skin and venereal diseases, no matter what age they occur, based on professional knowledge of the semiotics of dermatoses and sexually transmitted diseases, and the ability to use special methods of nosological recognition. Knowing the basic etiological and pathogenetic methods of treating dermatoses, a dermatovenerologist must determine the stages of therapy, use different options for special treatment with a variety of topical agents, and carry out rehabilitation. According to the professional and job requirements for a specialist, every dermatovenerologist should know pediatric dermatovenerology, since there is no separate specialty in this discipline. In practice, this section, especially skin pathologies in children of the first year of life, turns out to be the most difficult for a dermatovenerologist. Based on the experience of the Department of Dermatovenerology of the Russian Medical Academy of Postgraduate Education and the children's department of the Moscow Clinical Dermatovenerological Hospital No. 14, we propose to discuss some issues related to this area.
Table 1. Diagnosis of dermatoses in infants and auxiliary studies
| Basic methods | Additional events |
| Inspection and clinical and morphological analysis of loose elements and technical techniques: | Pathological studies of skin biopsy: |
| Sweating tests | Histological |
| Examination under Wood's lamp | Ultrastructural |
| Others | Immunofluorescent |
| Taking anamnesis: interviewing relatives and persons caring for the child | Cytological fingerprint analysis |
| Examination of blood relatives examination of contact persons | Hemogram |
| Microscopic and cultural examination of material from lesions | Analysis of urine: |
| Complex of serological reactions to syphilis | General |
| Clinical assessment of general condition | According to Nichiporenko |
| X-ray of bones in congenital syphilis, malformations, proliferative diseases | Stool analysis: For scatology For helminths For dysbiosis |
| Biochemical blood tests | |
| Paracoagulation tests | |
| Immunogram (T-lymphocytes and their subpopulations, IRI, B-cells, lgG, lgM, lgA; circulating immune complex, complementary blood activity, phagocytosis activity) Level of total lgE and allergen-specific antibodies (PAST; determination of precipitating lgG antibodies) Special biochemical, karyological, immunological tests for suspicious clinical syndromes with dermopathy Determination of the sensitivity of flora from skin lesions to antimicrobial agents |
DIAGNOSTIC PRINCIPLES AND METHODS OF EXAMINATION
The main reason for diagnostic errors is the underestimation of the information content of the data that can be obtained using clinical and morphological analysis of skin lesions, which is a specific diagnostic method in dermatology. Dermatological examination
consists primarily of
a visual examination with
a detailed interpretation of the primary and secondary eruptive elements, supplemented by simple tests to identify a number of symptoms (Nikolsky, Unna-Daria, symptoms of the psoriatic triad, areas of loose hair, etc.) and such simple technical techniques as scratching, diascopy, examination under a Wood's lamp, hair microscopy, examination of the functions of the skin glands, analysis of the scalloped skin pattern, etc.
Under a Wood's lamp, you can not only see the green glow of hair in microsporia, which is detected in some children as early as 3 months of age, or the red fluorescence of the cystic fluid in congenital erythropoietic porphyria, but also examine weak inflammatory and dyschromic lesions that are invisible in normal lighting spots, the identification of which is extremely important for the early diagnosis of phakomatoses, since white spots and pigmentation in the first year of life may be the only visible signs of these dangerous diseases. The results of sweat tests
can also be vital revealing anhidrosis, which without appropriate correction will lead to severe disturbances in thermoregulation, febrile convulsions and even more tragic consequences of undetected malformations, accompanied by hypoplasia or dysfunction of the sweat glands.
Microscopic examination of the hair shaft
makes it possible to reliably diagnose Netherton's syndrome and many other diseases characterized by congenital hair abnormalities, some of which are associated with immune and mental disorders.
Table 2. Skin changes and lesions in newborn infants.
| Physiological and transitional states in newborns | Pathological processes |
| Original lubricant* | Erythema toxicum of the newborn* |
| “Lullaby cap” (remnants of grease on the head)* | Transitory edema* |
| Physiological skin catarrh* | Vascular changes of harlequin type* |
| Physiological peeling* | Scleredema* |
| Sebaceous ichthyosis* | Sclerema* |
| Lanugo-primary hair* | Adiponecrosis of newborns* |
| Yellow line of the abdomen* | Infantile seborrheic dermatitis |
| Neonatal telangiectasia* | Congenital genodermatoses |
| Neonatal hyperhidrosis* | Diaper rash |
| Miliaria uncomplicated | Diaper dermatitis |
| Perenial dermatitis | |
| Miliaria complicated | |
| Vesiculopustulosis | |
| Pyococcal pemphigoid | |
| Ritter's exofolitative dermatitis |
Notes. An asterisk indicates conditions and skin diseases specific to the neonatal period.
Table 3. Manifestation of hormonal crisis.
| Skin | Other |
| Increased sebum secretion | Breast engorgement |
| Gneiss | Desquamative vulvovaginitis |
| Milia-retention sebaceous cysts | Hydrocele |
| Focal pigmentation | Prostatitis |
| Reducing resistance to lipophilic flora | Hyperemia and swelling of the skin of the external genitalia |
In the absence of such structural abnormalities, syphilitic alopecia should not be forgotten in the differential diagnosis. Additional information for early diagnosis of dysplastic genodermatoses and hereditary keratinization disorders will be provided by examination of the scalloped skin of the palms and soles. In this case, not only anomalies of flexor folds in the form of dysmorphogenetic stigmas can be identified, but also pathogenetic signs of impaired formation of papillary patterns, included in the core of the syndrome in some developmental defects. The characteristic high intensity of additional folds on the scalloped skin in the first months is often the only sign of vulgar autosomal dominant ichthyosis, while obvious peeling occurs towards the end of the year or later. The symptom of lacquered pads on the fingertips, almost devoid of epidermal ridges, which is especially pronounced in the first months of life, is characteristic of lamellar ichthyosis; gross deformations of flexor folds are typical of diseases accompanied by the intrauterine formation of rough and constricting hyperkeratotic layers. Already in the second half of the first year of life, the disappearance of papillary patterns after the resolution of the blisters can be clearly observed, which is an important sign that allows one to differentiate dystrophic epidermolysis bullosa from other types and determine the prognosis. In some cases, it is necessary to resort to vitropression and use a button probe, since in the first year, children with tuberculosis may develop not only erythema nodosum, but also, in rare cases, acute disseminated miliary tuberculosis of the skin. Through vitropresion
Characteristic yellowish-brown small spots can be detected in the case of sarcoidosis; differences in color on diascopy will allow differentiation of vascular spots and hemorrhages, deep-pigmented spots and anemic nevus.
The dermatologist should constantly use the scratch technique to identify not only Auspitz phenomena, but also hidden peeling in various dermatoses, as well as purpura, serous wells, and acantholysis. Taking an anamnesis and examining relatives
constitute the next stage of the examination.
The anamnesis is often uninformative, the patient cannot yet make complaints, and parents do not always carefully record the dynamics of the disease. It is all the more important at this age to complete the clinical and morphological analysis and family examination. When examining blood relatives, you can obtain the necessary data to confirm or exclude mendelian dermatosis. As for multifactorial dermatoses, genealogical information is important for their scientific study, but has no practical diagnostic value, since at the time of examination a relative may be in remission, and anamnestic indications are inaccurate; in addition, there is no such alternative sign as a different type of inheritance for monogenic diseases. Examination of relatives and other persons in close contact with the child is more necessary when identifying infectious or parasitic dermatosis, both to confirm the diagnosis and to prescribe effective treatment and preventive measures, however, a special need to examine the mother arises if there is a suspicion of blenorrhea, syphilitic pemphigus, diffuse Hochsinger's infiltration, osteochondritis, coriza or other lesions that may be associated with sexually transmitted diseases. Among laboratory tests,
to establish a diagnosis in the case of a suspicious clinical picture, tests confirming candidiasis or other fungal infections, scabies, and sexually transmitted diseases are required.
Pyoderma is usually diagnosed clinically, but other bacterial dermatoses should be considered. For example, if impetigo does not heal within a week with adequate treatment, it is imperative to perform tests to exclude skin diphtheria. Pathomorphological examination
of the skin is carried out in exceptional cases; it is indicated for tumors, sarcoidosis, lymphomas, Curt-Macklin spiny ichthyosis, for the differential diagnosis of nosological forms of epidermolysis bullosa.
You can perform a simple cytological analysis
of fingerprint smears from the erosion and the bottom of the bladder.
In children with pigment incontinence, 50% of eosinophils are found in the contents of the bladder. There are few other indications, since dermatitis herpetiformis with an early onset at the end of the first year of life is extremely rare, and juvenile pemphigoid and familial pemphigus Hailey-Hailey develop later. It is possible to identify differences between staphylococcal scalded skin syndrome and Lyell's syndrome: in the first, blisters occur in the granular layer of the epidermis, in the second - in the basal layer, although the diagnosis is usually made on the basis of the clinical picture. The importance of x-ray examination
of long bones in the first 3 months of life, when osteochondritis can be detected, which (at 11-111 degrees) is a reliable sign of early congenital syphilis, which is especially significant when its other signs - visceral lesions, even multiple foci of diffuse infiltration of the skin - are interpreted incorrectly and are not made serological tests. Bone radiography should be ordered when clinical signs of mastocytosis or Abt-Letterer-Siwe disease appear to determine the shape or extent of the lesions. X-rays of the jaws are of great diagnostic importance if Christ-Siemens syndrome is suspected.
Table 4. Particularly dangerous dermatoses or their episodes in newborns and infants
| Infections | Epidemic pemphigus of newborns |
| Staphylococcal scalded skin syndrome (Ritter von Rittershein's exfoliative dermatitis of neonates) | |
| Gangrenous erysipelas | |
| Gangrenous ecthyma | |
| Generalized chronic candidiasis | |
| Kaposi's eczema herpetiformis | |
| Infantile papular acrodermatitis (Gianotti-Crosti syndrome) | |
| Immune diseases and toxic reactions | Stevens-Johnson syndrome |
| Lyell's syndrome - toxic epidermal necrolysis | |
| Plasma-associated phagocytosis defect (Leiner's desquamative erythroderma) | |
| Exfoliative erytoderma of any etiology (toxic, drug-induced, lymphoblastic) | |
| Hereditary diseases | Atopic erythoderma Hill |
| Congenital monogenic dermatoses with generalized inflammatory, bullous, keratotic skin lesions | |
| Acrodermatitis enteropathica | |
| Diseases of unknown etiology | Sclerema of newborns |
| Scleredema of newborns | |
| Systemic mastocytosis (cutaneous-visceral) |
The above practically exhausts the range of basic studies necessary to establish a nosological diagnosis. However, to assess the severity of the condition, the presence of background disorders and intercurrent diseases, a number of laboratory tests are required,
the minimum list of which is given in table.
1. Additional studies also include some etiologically significant measures (skin biopsy examination, special tests for secondary dermopathy)
due to the rare need or inaccessibility in a dermatovenerological hospital or clinic. Attention should be paid to the need for frequent repetition of urine tests for microbial dermatoses and atopic dermatitis due to the risk of developing acute pyogenic nephritis and membrane-destructive processes, monitoring the immunogram during immunocorrective therapy, determining average weight peptide molecules and other indicators of endogenous intoxication in children with complicated atopic dermatitis and other severe dermatoses. A high level of endotoxemia is also reflected in mesenchymal, liver and paracoagulation tests, protein and hemogram. A blood test for sugar may be urgently required during treatment with glucocorticosteroids in patients with severe dermatoses; hypoglycemia and hypothalamic insufficiency are possible in seriously ill children, including those with early congenital syphilis.
Table 5. Diseases with bullous eruptions.
| Infections and intoxications | Monogenic dermatoses and diseases of unknown etiology |
| Syphilitic pemphigus | Bullous ichthyosiform erythroderma |
| Pyococcal pemphigoid | Pigment incontinence |
| Staphylococcal scorched skin syndrome | Acrodermatitis enteropathica |
| Dyell's syndrome | Congenital erythropoietic porphyria |
| Stevens-Johnson syndrome (herpes-associated and other variants) | Hereditary epidermolysis bullosa |
| Fixed drug rash | Bullous forms of mastocytosis |
| Dermatitis herpetiformis |
AGE DYNAMICS OF SKIN PATHOLOGY IN THE FIRST YEAR OF LIFE
Brief information on this issue can help in the diagnosis of dermatoses in newborns and infants. It is customary to talk about the atypicality of rashes in children of the first year who have psoriasis, atonic dermatitis, scabies, mycoses, etc. In fact, they seem atypical only to a doctor accustomed to adult patients. A more pronounced exudative component of lesions, small rash elements, localization features determined by the properties of the skin at this age and endogenous factors - this is what is typical for young patients, as well as the age-related dynamics of the disease picture and the nosological profile of the pathology. Age at the onset of the disease and the appearance of age-dependent symptoms are of great diagnostic importance. Not only the onset, but also the duration, as well as the general possibility of the occurrence of some dermatoses are limited to certain periods. For example, Leiner's disease and infantile seborrheic dermatitis are observed only in the first quarter of the year, while the onset of atonic dermatitis often occurs at the age of 3 months. At birth, the skin can only show manifestations of so-called congenital diseases, which begin to form during intrauterine development. These include some genodermatoses and rare cases of transplacentally acquired infections. Other diseases appear later, after a few hours, days, weeks, and sometimes in the second half or at the end of the first year of life. It is customary to distinguish between pathology and special conditions of the neonatal period. A number of those listed in table. 2 changes are observed only at this time, sometimes within just a few days (toxic erythema) or weeks (scleredema, sclerema), others resolve longer (adiponecrod, telangiectasia), others will last a lifetime (genodermatoses), infectious, irritative, traumatic lesions can occur at any age, but often in a different form. At the 1st - 2nd week of life, the newborn begins to show signs of a hormonal crisis (Table 3), which can last up to 3 months until the metabolites of fetoplacental hormones are eliminated. With proper care and the exclusion of drugs and products in the child and nursing mother, the metabolism of which is associated with the glucuronidation reaction (sulfonamide drugs, chloral hydrate, caffeine, alcohol), the manifestations of a hormonal crisis gradually disappear without treatment. Complications that sometimes arise are mainly associated with inadequate therapeutic effects and refusal to bathe the child, which contributes to the development of microbial skin lesions. At the end of the 1st month, many children develop manifestations of infantile seborrheic dermatitis in areas of the skin with increased sebum secretion, primarily on the head in the gneiss area, behind and in front of the ears, on the brow ridges, where accumulations of fatty yellow scales are visible against the background of erythema. Erythema-squamous lesions can also appear in the inguinal, femoral folds, and on the neck. With the end of the hormonal crisis, all seborrheic manifestations disappear, but untreated microbial complications may persist. In newborns and early infants, lesions called staphylococcal and candidal flora are common, colonizing integumentary tissues that have not yet been colonized by protective flora. They are especially dangerous in case of insufficient immunity and the presence of an entrance gate, especially an infected umbilical wound. In newborns, yeast stomatitis, sometimes intertriginous candidiasis of the folds, candidiasis of smooth skin, pseudopustular dermatitis of the trunk, vulvar candidiasis, and balanoposthitis often occur. The ducts of the sweat glands are often infected with staphylococcal flora, periporitis (vesiculopustulosis) occurs, which is facilitated by neonatal hyperhidrosis and miliaria, overheating, and poor care. With deeper inflammation of the sweat glands, multiple abscesses develop (pseudofurunculosis); they rarely appear in the neonatal period and are more common in children 3–7 months old. A specific form of staphyloderma in the neonatal period is epidemic pemphigus of newborns, which occurs on the 3rd - 5th day after birth or in the first 2 weeks in the form of multiple conflicts, leaving erosions with fragments of tires and crusts. Unlike syphilitic pemphigus, which can appear at the same time mainly on the palms and soles, pyococcal pemphigoid of newborns mainly affects the skin of the torso and very rarely the palms and soles. Less common at an early age is streptococcal infection in the form of erysipelas, spreading mainly from the navel and proceeding severely, or in the form of papular-erosive streptoderma (syphil-like papular impetigo). Similarities with syphilitic rashes are seen in the appearance of large dense papules, which, however, after opening, conflicts on their surface quickly erode and are surrounded by a rim of exfoliated epithelium, and most importantly, are not accompanied by other clinical and laboratory signs of syphilis. Since papular-erosive streptoderma affects the skin of the buttocks and adjacent areas, many identify it with diaper dermatitis. Others consider diaper dermatitis and diaper rash to be a traumatic lesion, which is often infected with streptococcal, candida and other flora (streptococcal and candida diaper rash). A characteristic symptom of diaper dermatitis is the smell of ammonia (ammonia dermatitis). In newborns, diaper dermatitis is rare, most often detected at 2 months of age, although it can be observed in children from 2 weeks to 8-9 months and is a typical disease of infancy. Diaper and seborrheic dermatitis are often combined with perianal dermatitis, which can occur in the first days of life or from the 2nd week and, according to the literature, lasts 7 - 8 weeks (however, we observed it later, even in children older than 1 year suffering from atopic dermatitis and intestinal dysbiosis). In the second half of the first year of life, other forms of streptoderma are more often observed: bullous and periungual impetigo, interginous streptoderma in the postauricular and other folds, later erythematous-squamous streptoderma, and in weakened sick children with poor care - ecthyma. Viral diseases appear, most often molluscum contagiosum, less often - herpetic infections. All types of microbial skin lesions can complicate the course of atopic dermatitis, the most common disease in the second half of the first year of life. Allergic dermatitis is rare, but simple contact dermatitis, resulting from the irritating effect of care products containing detergents and disinfectants, saliva, and diapers, is quite common. Skin lesions become more noticeable after sun exposure in patients with xeroderma pigmentosum, erythropoietic porphyria, and congenital erythema telangiectatica with dwarfism (Blum's syndrome). Hereditary poikilodermic and telangiectatic syndromes and phakomatoses, hereditary palmoplantar keratoderma, atrophying keratosis pilaris, which is often mistaken for “diathesis,” hair shaft dystrophies, congenital pachyonychia, and variable erythrokeratoderma are manifested. When the child begins to crawl and stand, blistering lesions appear for the first time or worsen in some epidermolytic types of epidermolysis bullosa. In the second half of the first year, secondary damage to epidermolysis bullosa (milium-like epidermal cysts, scars, changes in nails) becomes more distinct, the presence or intensity of which makes it possible to differentiate its numerous nosological forms (more than 20 diseases) with some certainty. In some diseases, different age-dependent signs and stages of development of the clinical picture consistently appear throughout the year. In Bloch-Suliberger syndrome, linear bullous lesions that occur in the first days and weeks against the background of erythematous and urticarial exanthema are already replaced in the first months by a hypertrophic stage with warty and lichenoid rashes, and after 6 months symptoms of the pigmentary and atrophic stages are formed. Between the 6th and 7th month, the picture of epidermolysis bullosa herpetiformis Dowling-Mehr, a frequently occurring but rarely recognized nosological form, becomes pathognomonic. In the first days, the newborn has blisters on the fingers and toes, then on the palms and soles, from the 2nd month - outbreaks of vesicular rashes on the face and in the submandibular area, between the 2nd and 6th months the appearance of blisters of a somewhat proximate nature is noted. smaller than the palms and soles, and after 6 months, spreading to the skin of the extremities, the blisters form distinct herpetiform groupings with central healing, which is an important differential diagnostic feature, very clear in subsequent years, when a herpetiform rash appears on the body. The high diagnostic value of age-dependent symptoms and the dynamics of the appearance and frequency of different groups of diseases is due to the fact that they not only complement the picture of the disease and the number of positively considered signs, but can also play the role of negative signs that reliably exclude one or another proposed diagnosis.
SEVERE, DANGEROUS AND ACUTE PROCESSES
It is always necessary to remember that infants can develop severe skin diseases, sometimes with lightning-fast dynamics, the prognosis for life of which is uncertain if medical care is untimely. They can be associated with infection or intoxication, an unusual reaction of the body, immune disorders or genetic defects. The most well-known and significant diseases are presented in table. 4. Scleredema and sclerema, which develop in the 1st week of life, sometimes from the 2nd to 3rd day, and are manifested by swelling of the subcutaneous tissue, have some similarities, but their prognosis is different. Scleredema is considered as a cold injury of newborns against the background of a number of disorders and diseases of the child or mother; among the complex of therapeutic measures, warming is important. Sclerema, which develops in premature, weakened, malnourished and dehydrated children, can be fatal; glucocorticosteroid hormones and symptomatic drugs are used in its treatment. Pyococcal pemphigoid and erysipelas are especially severe in newborns against the background of omphalitis and umbilical sepsis. Exfoliative dermatitis of newborns, described by Ritter in 1878, was considered a malignant variant of pyo-coccal pemphigoid. Now it is identified with staphylococcal burnt skin syndrome, which can occur at an older age, but in newborns in the 1st week of life it is especially severe, accompanied by high temperature and intoxication. Beginning with cracks and redness of the skin near the navel and mouth, a sudden eruption of large superficial blisters, the lesion within a few hours takes on the character of generalized hyperemia with swelling, erosion, with detachment of the epidermis resembling a burn, with a positive Nikolsky sign. The cause of this acute toxic skin lesion is associated with exposure to epidermolysins secreted by phage group II Staphylococcus aureus and the presence of an active focal infection in the upper respiratory tract or other organs. Skin lesions are quickly controlled by systemic administration of antibiotics. Leiner's disease begins after 3 weeks of age, is acute and severe, manifested by widespread erythema and desquamation, diarrhea, and severe malnutrition. The cause of the disease is considered to be congenital immune deficiency, accompanied by a decrease in the opsonic activity of serum against yeast-like fungi, impaired phagocytosis, and deficiency of complement component 5. In stool tests, staphylococci, gram-negative flora, and yeast-like fungi are detected in patients. After the 3rd month of life, this disease does not occur. Toxic epidermal necrolysis and Stevens-Johnson syndrome are observed at any age, but, unlike staphylococcal scalded skin syndrome, they occur less frequently in children of the first year of life than in adults, although cases of Lyell's syndrome have been described even in newborns. It can develop as early as 2 days after taking a drug that caused a specific autoimmune reaction against epidermocytes, although the average time is about 2 weeks. The danger and severity of this disease are associated not only with internal multisystem damage, widespread involvement of the mucous membranes (with staphylococcal burnt skin syndrome they are not affected), but also with the possibility of sepsis, since erosions are colonized by Staphylococcus aureus and gram-negative flora. Other bullous diseases also tend to be complicated by secondary infection, and there is a risk of pyogenic damage to the kidneys or other organs, but the frequency and severity of complications vary. To assess the prognosis and early initiation of adequate measures, it is necessary to have a clear understanding of the diseases listed in Table 5.
Conclusion
Reliable nosological recognition of skin diseases in newborns and infants must be carried out as soon as possible. This opportunity is ensured by visual accessibility of the organ, subject to professional performance of clinical and morphological analysis of eruptive elements, correct assessment of age-dependent symptoms, specific differential diagnosis within the nosological profile of each age segment, knowledge of the age-related evolutionary dynamics of skin pathology.
Literature:
1 . F. Zverkova. Skin diseases of young children. Saint Petersburg. - Sothis. -1994 — 235 p. 2. K.N. Suvorova, A.A. Antonev, N.P. Kuznetsova, I.O. Malova. Skin and venereal diseases in children. .Irkutsk, - Irkutsk University Publishing House. -1995. 3. Yu.K. Skripkin, G.Ya. Sharapova. Skin and venereal diseases. - M.: - Medicine. -1972. 4. Yu.K. Skripkin, F.A. Zverkova, G.Ya. Sharapova, A.A. Studnitsin. Guide to pediatric dermatovenerology. - A.; Medicine. - 1983.
Will there be complications after erythema toxica?
Erythema toxicum is not a disease. Whatever the cause of the rash, doctors call this physiological process a “borderline” state—it’s not even a “full-fledged” allergy. It does not harm the child’s health and does not cause any consequences. When the spots disappear, not the slightest trace remains on the skin, such as after chickenpox. Even in the case of generalized toxic erythema with ulcers, unevenness does not form on the skin.
Since the cause of the appearance of rashes in newborns still remains a “mystery of nature,” any preventive measures will be useless. In general, no child is “safe” from toxic erythema.
- share with your friends!