Patients who become infected with Demodex mites may experience unpleasant symptoms. Sometimes this disease leads to serious complications.
When a mite penetrates the eye area, it leads to increased tearing, eyelash loss, and inflammation. This parasite multiplies in the sebaceous and meibomian glands, as well as in the hair follicles of the patient. Often a tick infection is asymptomatic, that is, it does not cause any discomfort to the host. However, the activity of the tick can increase when the functioning of human internal organs is disrupted, including the immune, nervous and endocrine systems.
The size of the Demodex mite varies from 0.16 to 0.48 mm. About 25 individuals can live in one hair follicle. In a quarter of cases of tick detection on the skin of the face, damage to the sebaceous glands and meimobian ducts occurs. A number of ophthalmological problems are also caused by infection with this parasite. Thus, it is one of the leading causes of blepharitis, chalazion, blepharoconjunctivitis, episcleritis, and keratitis.
The cause of demodicosis is the acne iron mite
The demodex mite (D. follicullorum) belongs to the genus Demodex, family Demodicidae, suborder Trombidiformes, order Acariformes.
A little history
- The parasite was first discovered in 1841 by two independent researchers Henle (identified the parasite on human skin) and F. Berger (identified the parasite in earwax).
- In 1842, C. Simon identified mites in hair follicles and described the parasite for the first time. Between 1917 and 1923, acarologist Hirst identified 21 species and several subspecies of demodex mites in animals.
- In 1963, L. Kh. Akbulatova described a new species of iron mite, Demodex folliculorum brevis.
Spreading
Demodex mites are the most common parasites living on the surface of the body of humans and animals. They live in the mouths of hair follicles and the excretory ducts of the sebaceous and meibomian glands. Of the 100 known species of Demodex mites, 2 species live on human skin: Demodex folliculorum longus (long) and Demodex folliculorum brevis (short). Contamination of the skin occurs in childhood through contact. The maximum incidence occurs in females aged 20–40 years. At older ages, tick parasitism is registered in 80–100% of the population.
Acne iron mites live in places with high humidity; the parasites do not live long outside the host, are distributed everywhere, and are recorded in all races and in all geographical zones.
General characteristics of parasites
Acne gland mites live in the mouths of hair follicles and excretory ducts of the sebaceous and meibomian glands of the skin of the face (T-shaped zone), in the ears, and less often on the back and chest. There is an atypical localization of parasites.
Demodex mites feed on epidermal cells and sebum.
At night, ticks crawl to the surface to mate. Ticks move along the surface of the skin at a speed of 8 - 16 mm/hour.
At the head end (gnathosoma) there is a mouth opening equipped with sharp chelicerae that facilitate the absorption of food (epidermal cells and sebum). Digestion of food occurs under the influence of lytic enzymes.
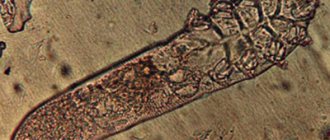
Rice. 2. Photo of demodex mites under an electron microscope.
Reproduction and development
Ticks crawl onto the surface of the skin at night to mate. That's when they end up with other hosts. The spring-summer period is the most favorable for parasites.
The life cycle of parasites is 14 - 18 days and consists of 5 developmental phases. After fertilization, the females return to the hair follicles and sebaceous gland ducts and lay diamond-shaped eggs, from which larvae emerge after 60 hours. In the developmental cycle, larvae transform from eggs, protonymphs and nymphs into adults. The appearance of a large number of parasites coincides with the first rashes on the skin.
Rice. 3. The photo shows (from left to right) the developmental stages of the demodex mite from egg, larva, protonymph and nymph to adult.
Features of Demodex folliculorum longus (long mite)
The tick of this species is long (0.3 - 0.4 mm), females and males are of the same size. The body is worm-shaped. The head end (gnatosoma), thorax (subsoma) and abdomen (opisthosoma) are well differentiated. The chelicerae of the oral opening are sharper.
The subsoma has setae. The covering (cuticle) is transparent. There are very short three-membered legs. Transverse striations of the posterior part of the body are noted. They live in hair follicles in groups.
Features of Demodex folliculorum brevis (short mite)
This species of tick has a short body (0.18 - 0.19 mm). The opisthosoma is short with a pointed cone-shaped end. The head end is short and flattened. Males are smaller than females and die after fertilization. The breast is wide and lacks setae. The cuticle is less transparent. They live in the mouths of the excretory ducts of the sebaceous and meibomian glands singly, which makes them difficult to detect. They rarely rise to the surface, making treatment difficult.
Demodex folliculorum longus is found 4 times more often in men and 10 times more often in women than Demodex folliculorum brevis.
Rice. 4. On the left are long demodex mites (Demodex folliculorum longus), on the right are short mites (Demodex folliculorum brevis).
Rice. 5. In the photo there is a short and a long demodex mite.
Reviews
Below are some reviews. If you have something to say, leave your feedback in the comments below the article, it will be useful to our readers.
“
I suffered from demodicosis once – after an unsuccessful outdoor recreation. I the symptoms literally on the second day , and at first I mistook it for conjunctivitis.But I was alarmed that the eyes themselves did not hurt or water, and pus formed only on the eyelashes.
During the examination, the doctor diagnosed the disease and prescribed metronidazole gel.
The treatment took about a month , after which the signs of the disease completely disappeared.”
Boris Shebanov, 38 years old.
“
My daughter became infected with demodicosis from one of her friends. The disease immediately manifested itself to the maximum:
the girl’s eyes itched, pus formed on her eyelashes every morning , and on her pillow I found fallen eyelashes for two or three days in a row, which had never happened before. The doctor recommended several ointments, including ichthyol ointment and demalan gel.The treatment was long (more than a month and a half), but with each week the improvements were evident.”
Snezhana Tsvirko, Pskov.
Epidemiology of demodicosis
Source of infection
The main source of demodex mites are sick people or carriers.
Distribution routes
- Iron mites can be transmitted through bedding, underwear, and personal items. The parasites were found in house dust, the source of which was bedding.
- Some researchers suggest that ticks can get on a child during breastfeeding from a sick mother.
Sustainability
Constant humidity, darkness and air temperature within 30-40°C are optimal conditions for iron mites. Outside the host, at room temperature, constant humidity and in the dark, ticks live up to 9 days.
According to the observation of some researchers, parasites remain viable in water for 7 days, and up to 2 weeks in immersion oil.
Rice. 6. Demodex mite under a microscope.
Reasons for the development of the disease
Keep in mind! Typically, pathogens such as demodex do not survive in the human body.
But they can become active and begin to reproduce under the following conditions that reduce the functionality of defense mechanisms:
- hormonal changes;
- constant presence of a person in conditions of elevated external temperature. For example, in areas with a hot climate or when constantly working in conditions of elevated ambient temperature;
- any ophthalmological and dermatological infectious and inflammatory pathologies;
- constant exposure to open sunlight.
Demodex can be transmitted by contact through household objects , but cases when the tick passes to humans from domestic and wild animals cannot be excluded.
How the disease develops
Demodicosis in humans can develop for the first time and occur as an independent disease, or develop against the background of existing skin diseases (acne, perioral dermatitis, rosacea, seborrheic dermatitis, etc.). From 55 to 100% of the population are carriers of iron ticks and do not have any manifestations of the disease, which proves that the parasites belong to the opportunistic flora. Damage to follicles by parasites increases with age.
Factors in the development of the disease
Acne iron mites are an opportunistic infection. They can parasitize a person for many years without causing him any harm. Their activation and active reproduction depends on a number of factors.
- Changes in microbiocenosis, the function of the sebaceous glands and the composition of sebum are the trigger mechanism of the disease. Changes in the composition of surface lipids lead to the development of dysbiosis.
- Demodex mites are carriers of viruses and microbes into the sebaceous glands and hair follicles. When pathogenic pyococci and fungi Pityrosporum spp are introduced, purulent-necrotic inflammation develops.
- The bacillus Bacilluss oleronius found on the surface of the parasite increases the activity of ticks and stimulates staphylococci, streptococci, acne propionobacteria, and fungi of the genus Malassezia to produce anti-inflammatory proteins, which triggers a cascade of immune reactions.
- The presence of foci of chronic infection, disturbances in the functioning of the liver and gastrointestinal tract, endocrine glands, nervous system, and corticosteroid therapy contribute to the activation of ticks.
- The rise in incidence in the spring-summer period is associated with increased insolation. An increase in the production of vitamin D under the influence of ultraviolet radiation leads to an increase in the synthesis of cathelicidins, which support the inflammatory process.
- The likelihood of infestation by Demodex mites increases in individuals with a sharply reduced functioning of the immune system, which occurs with primary and secondary immunodeficiencies, long-term use of corticosteroids and cytotoxic therapy, HIV infection, leukemia, T-cell lymphoma and other malignant neoplasms.
- The mite infestation maintains the activity of the existing inflammatory process. An imbalance in the cytokine cascade develops when the immune response is too strong.
Mechanisms of action of iron mites on humans
The impact of Demodex mites on humans is multifaceted:
- When feeding, the parasites secrete aggressive saliva and mechanically destroy the cell walls of the sebaceous glands and follicles, inflammatory infiltrates and granulomas form in the dermis, and the processes of keratinization and pigmentation develop.
- Substances formed after the death of ticks have antigenic properties, which leads to allergization and increased immune response.
- When the immune system is suppressed, opportunistic flora is activated, which successfully colonizes the host.
Acne iron mites act as carriers of bacteria and viruses, which complicates the course of demodicosis and complicates treatment.
Rice. 7. Histological preparation of a skin section. Arrows indicate the location of demodex mites.
Prevention
Unlike other parasites and bacteria in general, demodex is rarely activated in the body, and often the defense system fights it on its own.
But you can reduce the risk of tick damage by following these preventive recommendations :
- During the summer, swimming in unknown or polluted bodies of water should be avoided .
- Even members of the same family must use separate towels and bedding . This should be especially avoided in public places and when traveling.
- It is not recommended to come into too close contact with domestic and wild animals. This is explained by the fact that even if the animal itself is not sick, it may be a carrier of demodex, and this cannot be determined visually.
Important! After successful treatment, these rules should also be followed, since immunity to these mites is not developed, and each time the probability of developing the disease remains the same.
After treatment, repeated tests are always required to completely exclude the possibility of relapse of the disease in cases where a small number of parasites still remain in the follicles.
Clinical variants of demodicosis
Demodicosis in humans can develop as a primary independent disease, or it develops against the background of existing skin diseases (perioral dermatitis, rosacea, acne, seborrheic dermatitis, etc.), aggravating their course.
Primary demodicosis
In primary demodicosis, inflammatory skin elements resolve after antiparasitic therapy. About 40% of cases of primary demodicosis develop in patients suffering from rosacea.
Primary demodicosis is characterized by:
- the onset of the disease over the age of 40 years;
- The areas most often affected are around the mouth, eyes and outer ear;
- inflammatory elements are located asymmetrically and are accompanied by itching;
- acne and rosacea are absent;
- high content of mites on the skin;
- positive effect of the antiparasitic treatment.
Secondary demodicosis
Secondary demodicosis develops against the background of diseases accompanied by a sharp suppression of the immune system (HIV infection, leukemia, etc.), long-term use of corticosteroids and cytotoxic therapy, or develops against the background of acne and rosacea, complicating their course. This form of the disease is registered in 33% of patients with acne.
Secondary demodicosis is characterized by:
- the disease appears at any age;
- lesions are widespread;
- presence of anamnesis and clinical picture of relevant diseases.
Papulopustular rashes on the skin of the face are a reason for diagnosing demodicosis.
Rice. 8. Demodectic mange on a woman’s face.
Treatment methods
Stay up to date! Treatment is a long process that requires supervision by specialists and the development of an individual treatment regimen.
At the same time, during the treatment process, the patient must strictly observe the rules of personal hygiene : do not use other people’s utensils and washing products, wash your hands and face with soap more often, change bed linen every few days.
avoid decorative cosmetics during therapy .
Washing the patient’s linen should be done using disinfectants and in water at a temperature of at least 75 degrees.
Drug treatment
Drug treatment is the basis of therapy for demodex.
For this disease, both tablets and ointments and gels for external use are equally effective.
Signs and symptoms of demodicosis
The disease always occurs gradually and tends to spread and progress.
The main localization of demodex mites
Short mites live in the mouths of the excretory ducts and the secretion of the sebaceous glands of the skin of the face, ear canal, chest and back, sometimes on the scalp, as well as the meibomian glands, which are modified sebaceous glands that open at the edges of the eyelids. Long mites live in hair follicles. Mites were found on the penis, buttocks, and in the area of ectopic sebaceous glands.
Rice. 9. Demodectic mange on the face in the area of the nasolabial folds.
Rice. 10. Demodectic mange on a woman’s face in the chin area.
Rice. 11. Demodectic mange on the skin of the cheeks, nose and around the mouth.
Rice. 12. Demodectic mange on the face of women on the skin of the forehead, cheeks and nasolabial folds.
Rice. 13. Demodectic mange on the face of women.
Rice. 14. Demodectic mange of the eyelids.
Characteristics of the rash
- Initially, erythematous (red) spots appear around the mouths of the follicles. The rash is located asymmetrically and is accompanied by lamellar peeling.
- The appearance of the rash is accompanied by a feeling of heat, burning, crawling and distension.
- Very quickly, pink or red papules with a cone-shaped top and gray scales appear in the reddened area. Papulovesicles (a vesicle is a blister filled with clear fluid) or papulopustula (a pustule is a blister filled with purulent fluid) often appear.
- Inflammatory infiltrates and granulomas form in the dermis. The skin over the affected areas thickens and its elasticity decreases. A feeling of tightness appears. The affected areas are covered with serous, serous-sanguineous or purulent crusts. Over time, hyperpigmentation develops: the skin becomes brownish or yellowish-brownish in color.
- With the massive development of a pyogenic bacterial infection, large follicular pustules (purulent elements) appear at the site of inflammatory infiltrates. Over time, they spread into the deeper layers of the dermis, which leads to facial disfigurement.
- The clinical picture of demodicosis for different types of mites is somewhat different from each other. Thus, when Demodex folliculorum is affected, erythema and peeling (desquamation of the epithelium) are more often recorded; when Demodex brevis is affected, papulopustular elements are often recorded, which are often located symmetrically.
- With long-term (chronic) demodicosis, thickening of the skin, loss of elasticity, and a feeling of tightness appear. Bloody-purulent crusts are located against the background of hyperemic skin. When a pyogenic infection is attached, pustules and microabscesses appear. Dense infiltrates form in the deep layers of the dermis, disfiguring the face.
Rice. 15. Demodectic mange on a woman’s face, severe.
Deterioration in appearance creates aesthetic discomfort for the patient and leads to the development of neuroses and depression.
Forms of demodicosis in humans
Depending on the nature of the manifestations on the skin, several forms of demodicosis are distinguished, the symptoms of which are characteristic of the corresponding diseases. Not to be confused with these diseases!
Acneform form
The acneiform type of demodicosis is characterized by the appearance of papules and pustules on the facial skin, which are similar to acne.
Rice. 16. Demodectic mange of the face in women. Acneform form of the disease: papular (photo on the left) and papulopustular (photo on the right).
Rosacea-like form
The rosacea-like type of demodicosis is characterized by the appearance of papules against a background of diffuse erythema. Demodex brevis (short mite) causes the appearance of inflammatory infiltrates and granulomas in the deep layers of the dermis, which are similar to the granulomatous form of rosacea.
Rice. 17. Rosacea-like form of demodicosis: in the form of diffuse erythema (photo on the left), granulomatous form (photo on the right).
Seborrheic (erythemo-squamous) form
The seborrheic form of demodicosis is characterized by the appearance of redness and rash on the facial skin, accompanied by lamellar peeling.
Ophthalmic form
The ophthalmic form of demodicosis occurs with damage to the eyeballs and eyelids. Redness, dryness, irritation, sensation of a foreign body in the eye, fatigue are the main symptoms of eye demodicosis. Itching of the eyelids, redness and swelling of their edges, the appearance of scales or crusts on the eyelids are the main symptoms of demodicosis of the eyelids.
Read in detail in the article “Demodicosis of the eyelids and eyes”
Rice. 18. Demodectic mange of the eyelids. Lamellar peeling is clearly visible (photo on the left). On the ciliated edge of the eyelid, scales form a “collar” around the eyes (photo on the right).
The role of demodex mites in the formation of androgenetic alopecia
There is an assumption that the presence of mites in the hair follicles aggravates the development of androgenetic alopecia. During inflammation, T-lymphocytes are activated, which induce collagen synthesis, resulting in fibrous degeneration of hair follicles.
Rice. 19. Demodicosis of the scalp.
Demodectic mange against the background of rosacea
Demodicosis complicates the course of rosacea in 88.7%. The disease is more common in women over 30 years of age. The phymatous form of the disease is more common in men. The pathological process is characterized by redness of the skin of the face, associated with the expansion of small superficial vessels, the appearance of papules and pustules. Papules increase in size over time and merge, forming dense infiltrates. The sebaceous glands become hyperplastic. Fibrosis develops. Persistent redness and fibrous lumps on the nose are called rhinophyma.
There are many reasons for the development of diseases. Factors contributing to the development of the disease can be divided into endogenous and exogenous.
Rice. 20. Erythematotelangiectatic form of rosacea. Multiple telangiectasias (dilated subcutaneous arterioles) are visible on the skin.
Rice. 21. The photo shows the papulopustular form of rosacea. Against the background of erythema (redness), multiple rashes are visible, which are papules with thin scales on the surface. The affected areas are infiltrated and swollen.
Rice. 22. Demodex brevis (short mite) causes the appearance of inflammatory infiltrates and granulomas in the deep layers of the dermis, which are similar to the granulomatous (phymatous) form of rosacea. The photo shows the phymatous (papular-nodular) form of rosacea.
Rice. 23. Severe form of rosacea.
Rice. 24. The ocular form of rosacea is registered in 50% of patients. Inflammation of the eyelids, redness of the conjunctiva, iritis and keratitis are the main manifestations of the disease.
Demodicosis on the background of acne
Among acneiform dermatoses, demodicosis accounts for 10.5%. Acne (acne vulgaris) is a chronic, relapsing disease that affects the sebaceous glands and hair follicles. Most often, acne occurs in males during puberty between the ages of 14 and 16 years. The cause of juvenile acne is propionobacteria acne, epidermal staphylococci, pityrosporum ovale and orbitale, which constantly live on the skin of the face. Many factors contribute to the development of acne.
Rice. 25. Demodicosis is registered in 10.5% of patients with acne. The photo on the left is papular acne. When a staphylococcal infection is attached, pustules (ulcers) and microabscesses develop - pustular and abscess acne (photo on the right).
Rice. 26. With the indurative form of acne, inflammatory infiltrates appear in the deep layers of the dermis. The skin has a bumpy appearance.