HPV itself does not affect a woman’s ability to become pregnant, carry and give birth to a healthy child. But in the human body everything is interconnected, and one problem in most cases can lead to a number of others - the “domino principle” works. Therefore, in the case of a diagnosed human papillomavirus, it is recommended to regularly undergo immunological, gynecological and oncological examinations and treatment.
According to statistics, up to 30 percent of Russian women of reproductive age are exposed to the human papillomavirus (HPV). Therefore, it is important for every expectant mother to know how this virus can affect the ability to have children.
Victoria Viktorovna Zaletova, chief physician of the MAMA clinic:
“How to get pregnant with HPV? Is it possible to get pregnant with HPV?
- many women ask.
We answer:
It is generally accepted that the human papillomavirus does not affect a woman’s reproductive function. By itself, it really does not have any effect on the ability to become pregnant, bear and give birth to a child. But HPV is often the “tip of the iceberg”, under which many immune and gynecological problems are hidden.
The human papillomavirus, like any other virus, negatively affects the immune system. The immunity of an HPV-infected person is constantly in a depressed state, which means that he is more susceptible to infectious diseases, which can lead to a variety of consequences.
If we talk about pregnancy, then this is stress for a woman’s immune system. The embryo combines the cells of the mother (“its own”) and the cells of the father (“foreign”). The main task of the immune system is to fight “foreign” cells. But pregnancy is an exception, the body adapts, the immune system does not work at full strength and accepts the “stranger” for the whole 9 months.
Provided that the immune system is in order. If its functioning is disrupted, spontaneous abortion in the early stages is possible. Moreover, the woman herself may not know about her situation, and her body has already rejected the tiny embryo. In this case, we are talking about immune infertility. An immunologist and a reproductive specialist can help: they will conduct blood tests and recommend treatment that will allow the woman to become a mother.
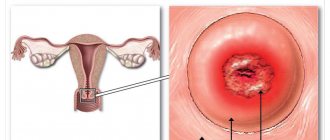
Human papillomavirus is a risk factor for the development of cancer. Moreover, the female reproductive organs take the hit: the cervix and uterus.
There are about 40 types of HPV that affect the mucous membranes of the genital organs and provoke gynecological diseases of varying severity.
Medical research has shown that HPV can cause benign lesions of the cervix and cervical cancer (some types of HPV).
Studies have also shown that certain types of HPV are detected in cervical intraepithelial neoplasia (CIN) and early stages of dysplasia.
Introduction
Infertility is a pressing medical and social problem.
In Russia, every fifth married couple is infertile [1]. Moreover, the male factor is responsible for half of these cases. This is associated with a progressive decline in reproductive function. There is numerous data on the negative impact of viruses on the state of the male reproductive system. Human herpes viruses (HHV) are widespread in the human population [2]. Herpes viruses cause lifelong infection and are the cause of many diseases, half of which have a relapsing course. From 95% to 100% of the population are infected with HHV, and at different periods of life a person is infected with at least one, and more often, several types of viruses belonging to the herpesvirus family. In the second half of life, almost all people have antibodies to most HHVs [3]. 8 types of herpes viruses are pathogenic for humans.
Own results
We conducted a study that included 287 men with chronic prostatitis/chronic pelvic pain syndrome IIIA, 23 of whom had infertility. Diagnoses were verified according to the criteria of the European Urological Association [30].
In addition to standard diagnostic procedures, HHV types 4–6 were detected in samples from the urethra, prostate secretion, and ejaculate.
When HHV was detected, patients with infertility (group 1) were prescribed valacyclovir 1000 mg/day for 3 months. and the drug VIFERON® (interferon α-2b in combination with antioxidants (vitamins E and C)) in the form of rectal suppositories. Based on the authors’ personal experience, patients were prescribed the following regimen of drug use: 3 million IU 2 times a day for 10 days, then 3 times a week (also 2 times a day) for the next 3 weeks. Viral load was monitored at the end of 3 months of treatment. The remaining patients in whom HHV types 4–6 were not detected (group II) were prescribed levofloxacin 500 mg for 30 days, tamsulosin 0.4 mg for 3 months, diclofenac suppositories 50 mg for 10 days.
In addition to the acyclic nucleoside, which has a direct antiherpetic effect and is prescribed for the treatment of abacterial prostatitis associated with herpes viruses, VIFERON® was chosen as a drug that can provide a long-term antiviral effect. The drug contains interferon α-2b, which is a human recombinant analogue of a substance produced in any cells of the body. It has antiviral, immunomodulatory, antiproliferative properties, suppresses the replication of RNA and DNA viruses. Interferon α-2b in cells triggers a sequence of reactions leading to suppression of the synthesis of viral proteins, assembly and release of virions into the intercellular matrix. In addition to influencing protein synthesis, interferons have epigenetic activity, activating hundreds of genes that play an important role in the antiviral defense of the cell [31]. In addition, interferon α-2b limits the spread of viral particles by activating the so-called “genome guard” protein p53, which leads to apoptotic death of the infected cell [32]. Ascorbic acid and α-tocopherol acetate, which are part of the drug, are highly active antioxidants, have anti-inflammatory, membrane stabilizing, and regenerating properties.
In 11 patients with identified herpes viruses, electron microscopic examination of sperm was performed (JEM 1400, JEOL, Japan).
We noted that out of 103 patients with detected HHV types 4–6, 8 had infertility (group I), while among 184 patients without herpes viruses, infertility was verified in 15 (group II).
Of the 24 urogenital samples from 8 patients in group I, 12 virus-positive samples were obtained: 7 - ejaculate, 1 - urethral smears, 4 - prostate secretions. CMV and EBV were detected in 4 and 3 samples, respectively, including samples with combinations of 2 HHVs. HHV-6 was much more common - in a total of 7 samples out of all 12. The median viral load of herpes viruses types 4–6 was 1770 copies per 100,000 cells.
As a result of antiviral treatment, by the end of the 3rd month, control studies detected the virus in only 5 of 8 patients in group I, in whom herpes viruses were detected in 5 bioassays. At the same time, the median viral load in them decreased to 48 copies per 100,000 cells.
As a result of therapy for 6 months. after the end of treatment, pregnancy was observed in the spouses of 10 out of 23 men, who were distributed into groups as follows: 6 out of 8 from group I and 4 out of 10 from group II. Statistical analysis showed that differences in pregnancy rates reached significant significance between groups I and II (χ2 criterion value was 4.960, critical χ2 value at the significance level p=0.05 was 3.841, significance level p=0.026).
The effect of the course of antiviral therapy was also assessed by electron microscopy. A study of spermatozoa of 11 patients with infertility showed that if before treatment, HHV capsids of types 4–6 were found in 8 patients, then after treatment in 4 of these patients, viral capsids were no longer detected in spermatozoa, and in 3 other patients the number of spermatozoa with capsids was on average decreased by more than 2 times: from 12% to 5% of infected gametes in the ejaculate (Fig. 1).
When should you start preparing for fertilization?
Often, conception occurs spontaneously. In such cases, men still need to undergo a series of tests. The most important thing is to identify the risks of hereditary problems in the male line. If they are present, then partners should consult a geneticist and undergo genetic screening.
If we talk about a responsible approach to family planning, then for men preparation for the intended conception begins at least 3 months in advance. This period was not chosen by chance. This is due to the maturation of sperm, the full cycle of which lasts approximately three months. If during this time the male body was exposed to negative effects, this will be reflected in the spermogram analysis.
Examination for both partners
In preparation for pregnancy, the following tests are taken:
- urine test - shows the degree of kidney function. Based on the presence of protein, leukocytes, pus, and red blood cells in the urine, inflammation in the genitourinary area and hematuria are detected;
- group and Rh factor - incompatibility of parents by blood leads to Rh conflict during gestation if this indicator in the child is not the same as in the mother. This can have a negative impact on the pregnancy itself and the health of the newborn. The problem manifests itself as hemolytic jaundice. The condition is not life-threatening if doctors are aware of this fact and can correct it in time;
- General blood test - allows you to identify infectious processes, anemia;
- blood biochemistry - gives an idea of the functioning of internal organs;
- glucose test - if glucose values are elevated or too low, a repeat test is performed. If it also showed poor results, then you need to consult an endocrinologist;
- blood for hepatitis C, RV, HIV, TORCH infections. Pathologies such as rubella, toxoplasmosis, cytomegalovirus, and others can be life-threatening for the fetus and mother;
- FLG - shows the absence of foci of tuberculosis in the lungs. If a pathology is suspected, the patient is referred to a phthisiatrician. Tuberculosis is a highly contagious infectious disease. It is dangerous to carry and give birth with such a disease. Even if it is not the pregnant woman who is sick, but the man who is next to her, this poses a great danger. In this case, hospitalization, special tests, and long-term treatment are required. Only after recovery can you plan for procreation;
- ECG - shows the state of cardiac activity.
Preparation for analysis is minimal. The night before, you cannot eat after 19:00 or drink alcohol. They come to the laboratory where venous blood is collected on an empty stomach. You must bring your urine with you for analysis. It is required to collect at least 50 ml in a sterile container. morning urine, preferably a medium portion. If general tests reveal deviations from the norm, then additional diagnostics are prescribed. The examination package is selected depending on the identified violations.
Diagnostics for men
If standard tests are normal and conception has occurred successfully, then the pregnant wife remains to be observed by a gynecologist throughout the gestational period. But it is not always possible to get pregnant. In this case, in-depth analyzes are required. A man must also undergo them, since in almost half of the cases the cause of infertility is the male factor. Most often, the problem is a violation of spermatogenesis.
When planning a pregnancy, a man needs to undergo the following tests:
- PCR test - a urethral smear is taken to detect the presence of pathogens that cause STDs. For non-advanced forms of STIs, it is enough to eliminate the infection to restore fertility.
- Spermogram - a semen analysis is prescribed if infertility is suspected. It allows you to determine the type of infertility and prescribe treatment. During the diagnosis, the quality of gametes and their quantity are assessed. The test is performed by masturbation in a specially designated clinic room. The sperm must be collected in a labeled container and immediately transferred to a laboratory assistant.
- MAR test – sperm morphology according to Kruger. The shape, size, and integrity of germ cells are assessed. The analysis shows such anomalies as the absence of a tail of the sperm, a double head, an elongated or shortened shape of the sperm. With such deviations, natural conception is unlikely. The couple may be offered in vitro fertilization or IVF with ICSI. These ART procedures offer a high chance of pregnancy if the woman is healthy.
- TRUS - sonography of the prostate gland. An ultrasound examination will show prostatitis and neoplasms. For example, an adenoma can cause mechanical obstruction of the vas deferens. Removing the formation will normalize the passage of sperm through the genital tract.
- Analysis of prostate fluid - microscopic examination of prostate secretion allows you to detect inflammation and evaluate the function of the gland.
- Blood test for hormones - a man donates material to determine follicle-stimulating, luteotropic hormones, prolactin, androgens, thyroid hormones. Testosterone is especially important. In women, the level of gonadotropins and gonadosteroids depends on the menstrual cycle. Therefore, they are assigned a specific day for analysis.
Men are not required to adhere to strict deadlines. They can take the test on any calendar day. Before the analysis, you cannot have sex for 3-4 days, you need to avoid stress. Upon arrival at the laboratory, you should rest and calm down. The stability of hormonal levels depends on the emotional state. Taking a test when you are worried may give unreliable results. There is a type of infertility called hormonal. These hormones influence spermatogenesis. Timely hormone therapy will help correct the situation.
When planning a pregnancy, examination of men is necessary for:
- determining the suitability of seminal fluid for fertilizing an egg;
- detection of infectious agents in reproductive and other organs;
- identifying genetic risks with a complicated medical history, as well as for people aged 40 years and over.
The list of tests is determined for each specific case.
Normal spermogram results
Main characteristics when analyzing ejaculate
Preparing for pregnancy with infectious pathology of the female reproductive system
The introduction of modern technologies into clinical practice has made it possible to expand research and show that the negative impact of environmental factors on the microflora of the macroorganism leads to a variety of pathologies of both inflammatory and non-inflammatory origin. Despite significant advances made in the diagnosis, treatment and prevention of sexually transmitted infections, their frequency does not have a clear downward trend. The latter is also associated with the increase in immunodeficiency conditions against the backdrop of deteriorating environmental conditions, poor nutrition, frequent stress, a pharmacological boom with the uncontrolled use of drugs, primarily antibiotics, etc. Most often, sexually transmitted infections are caused by several pathogenic factors - viruses, microbes, fungi , protozoa, which cause diseases similar in clinical course, but different in pathogenesis and treatment methods.
Participation in the formation of inflammatory diseases of the pelvic organs, accompanied not only by vaginal dysbiosis, but also by similar changes in the gastrointestinal tract and urinary system; psycho-emotional disorders; the formation of immuno- and interferon-deficient states - this is not a complete list of problems characteristic of patients with urogenital infections. These features are at the same time a pre-gravid background, which is not able to ensure the development of adequate compensatory and adaptive reactions necessary for the gestational process in the majority of these patients.
However, works devoted to the issues of preparing women with bacterial and/or viral infections for pregnancy are extremely few in number and are usually aimed at correcting individual parts of the pathological condition.
Based on the above, the most important and integral stage is the correct pre-conception preparation of women. Therefore, measures to combat infection must begin before pregnancy.
Stages of infection control measures
1. Detection of the following diseases in women:
- chronic inflammatory diseases of the appendages and uterus, ectopia of the cervix, frequent recurrent colpitis;
- developmental anomalies and chronic inflammatory diseases of the urinary organs, dysuric disorders of unknown etiology;
- sexually transmitted diseases (herpes, cytomegalovirus, chlamydia, mycoplasmosis, ureaplasmosis, candidiasis, etc.);
- chronic extragenital foci of infection with frequent relapses;
- tendency to frequent acute respiratory viral infections;
- reproductive dysfunction (infertility, ovarian dysfunction, spontaneous miscarriages, non-developing pregnancies);
- complicated course of previous pregnancies, childbirth, postpartum period (chronic placental insufficiency, chronic hypoxia and/or intrauterine growth retardation, premature birth, antenatal fetal death, anomalies of attachment and separation of placenta, purulent-inflammatory diseases of puerperia, etc.);
- adverse perinatal outcomes (intrauterine or neonatal infection, malnutrition or malformations of the newborn, disruption of the processes of early neonatal adaptation and/or subsequent physical and neuropsychic development of the child).
2. A thorough clinical and laboratory examination of women at risk to verify genital or extragenital infection, regardless of the level of damage to the reproductive system, using at least two modern laboratory diagnostic methods, a study of immune and interferon status, etc. 3.
Conducting complex treatment, which should include both etiotropic types of therapy (complex of antibacterial or antiviral treatment), and treatment of concomitant diseases.
4. Planning and preparation for pregnancy.
When a herpes viral infection is detected, it is treated with subsequent prevention of relapses.
For genital herpetic infection, regardless of the level of damage to the reproductive system, both basic (antiviral) therapy and treatment of concomitant diseases are indicated.
Basic types of treatment
The most modern and effective antiviral drug is valacyclovir. Valacyclovir is a prodrug, the L-valine ester of acyclovir. After absorption into the blood, valacyclovir is almost completely converted to acyclovir under the influence of the liver enzyme valacyclovir hydrolase.
a) The resulting acyclovir penetrates into cells affected by the virus, where, under the influence of the viral enzyme thymidine kinase, it is converted into monophosphate, then into diphosphate and active triphosphate. Acyclovir triphosphate inhibits DNA polymerase and thereby disrupts DNA replication of the herpes simplex virus. Consequently, the high selectivity of valacyclovir for tissues affected by the virus is explained by the fact that the first step of the phosphorylation reaction chain is mediated by an enzyme produced by the virus itself. Valaciclovir is prescribed 0.5 g 2-3 times a day for 5-10 days. The duration and dose of the drug are selected individually, taking into account the form and severity of the viral disease.
b) Against the background of blockade of virus replication - stimulation of nonspecific resistance of the body, depending on the indicators of the immune and interferon status of patients (immunoglobulin preparations, interferon inducers, enzyme therapy, etc.).
c) Simultaneous or sequential use of specific antiherpetic immunoglobulin 3.0 ml intramuscularly once every 3–5 days, for a course of 5 injections.
d) Stimulation of the specific resistance of the body (subject to an increase in the inter-relapse period by 1.5–2 times) with a herpetic vaccine 0.25 ml intradermally into the arm 1 time in 3 days (5 injections in total), after which a break in treatment for 2 weeks and then another 5 injections of 0.25 ml once every 7 days. Revaccination course - after 6 months.
e) Local use of specific ointments (Zovirax, alpizarin, megosin, bonafton).
When diagnosing cytomegalovirus infection, etiotropic antiviral therapy is carried out. There are no clear recommendations for the prevention and treatment of CMV infection. An ideal antiviral drug should have high clinical efficacy, selectivity towards the virus, complete safety for the human body, and viruscidal effect. Due to the current lack of drugs that would fully meet the above requirements in relation to CMV, the prevention and treatment of this infection presents certain difficulties. Correction of immunity indicators and interferon status is mandatory.
For CMV infection, it is recommended to carry out a course of passive immunization with anti-cytomegalovirus immunoglobulin, 3 ml intramuscularly once every 3 days, for a course of 5 injections. More effective is normal human immunoglobulin 0.25 g/kg every other day intravenously, 3 injections per course. Immunomodulators (T-activin, cycloferon, immunofan) can be prescribed; the criterion for their effectiveness is the positive dynamics of cellular immunity indicators. Cytotect is also used (in the form of a 10% solution of immunoglobulin with a high content of anti-CMV IgG) intravenously at a dose of 2 ml/kg every 2 days up to 8–10 times under the control of serological parameters.
The use of interferons is promising - viferon 0.5–1 million IU 2 times a day in rectal suppositories for 15–20 days. It is advisable to include systemic enzyme therapy in the prevention and treatment of CMV infection (Wobenzym 5 tablets 3 times a day or Phlogenzym 2-3 tablets 3 times a day 30 minutes before meals for 1-1.5 months). In addition to treating herpes viral infection, additional therapy is indicated. Treatment of a latent chronic inflammatory process in the endometrium (viral-bacterial etiology) should be carried out against the background of basic therapy and be etiotropic and pathogenetically substantiated. Considering the prevalence of anaerobic-aerobic associations, as well as myco-, ureaplasma and chlamydial infections, the use of broad-spectrum antibiotics is indicated.
If urogenital chlamydia, mycoplasmosis and ureaplasmosis are detected, the following is prescribed: spiramycin 1 tablet (3 million IU) 3 times a day for 5–7 days; josamycin 500 mg 3 times a day for 5–7 days; azithromycin 1 capsule (250 mg) 1 time per day for 6 days.
It is advisable to combine etiotropic therapy for infectious pathologies of the reproductive system with the use of antioxidants - ascorbic acid (vitamin C) 50 mg and vitamin E 100 mg 3 times a day. It is also possible to use efferent treatment methods (plasmapheresis, endovascular laser irradiation of blood).
Particular attention should be paid to restoring the microecology of the genital tract, since complications of the gestational period and childbirth associated with various disorders of the vaginal microcenosis include the threat of miscarriage, spontaneous miscarriages, premature birth, chorioamnionitis, untimely rupture of amniotic fluid, the birth of children with low body weight, chronic hypoxia and/or signs of intrauterine infection, in the postpartum period the occurrence of wound infection of the birth canal, endometritis.
Violation of vaginal microcenosis is most often associated with bacterial vaginosis and/or candidiasis infection. According to the literature, 75% of women of reproductive age have at least one episode of vaginal candidiasis. Currently, 196 species of fungi of the genus Candida are known. Of these, more than 27 species are isolated from human mucous membranes. According to summary data, Candida albicans is found in the intestines of 20–50% of healthy people, on the oral mucosa in 20–60%, and in the vagina in 10–17% of non-pregnant women.
Vaginal candidiasis in pregnant women occurs on average in 30–40% of cases. Before childbirth, this figure can reach 44.4%. The goal of treatment for bacterial vaginosis and vaginal candidiasis is to restore the normal microflora of the vagina and inhibit the growth of microorganisms that are unusual for this microcenosis. There are many drugs and treatment regimens for vaginal dysbiosis. However, there is no optimal drug that would meet all the requirements and be 100% effective.
For bacterial vaginosis, the following drugs are used: dalacin vaginal cream (2% vaginal cream containing 100 mg of clindamycin phosphate) once a day for 3 days or tantum rose - vaginal douche - 2 times a day for 7-10 days.
Drugs for the treatment of vaginal candidiasis are divided into the following groups:
1. Antibiotics (nystatin, levorin, natamycin, amphotericin B).
2. Imidazoles (clotrimazole, ketoconazole, miconazole).
3. Triazoles (fluconazole (Diflucan, Fungolon), itraconazole).
4. Combined drugs (Polygynax, Klion D, Pimafukort, Macmiror complex).
5. Other drugs (dafnedzhin, polyvinylpyrrolidone iodate, griseofulvin, flucytosine, nitrofungin).
In the acute form of vaginal candidiasis, antimycotics are prescribed 1 vaginal suppository (tablet) once a night for 6 days, and in case of relapse of a chronic infection - in the same dosage for 9 days. At the same time, sexual rest is observed for 2–3 weeks, and the spouse is treated (local 1% Canison ointment or other antifungal agent).
The evolution of new antimycotics is moving towards the development of shorter courses of treatment. In this regard, a new era in the treatment of mycoses began with the introduction into clinical practice of once or twice administered oral antifungal drugs, the active substance of which is fluconazole. One of these drugs is Fungolon, which is one of the most effective and highly safe antifungal drugs due to its metabolic stability, rapid absorption due to good solubility, and minimal effect on enzymatic processes in the liver.
Fungolon belongs to the class of triazole compounds that inhibit the biosynthesis of fungal membrane sterols, disrupt the synthesis of ergosterol, as a result of which fungal growth is inhibited. It has been established that the drug is active against mycoses caused by opportunistic fungi, including the genus Candida. At the same time, fungolon selectively acts on the fungal cell and, unlike other antimycotic drugs, does not affect the metabolism of hormones, does not change the concentration of testosterone in the blood in men and the content of steroids in women, which eliminates the development of adverse reactions.
The drug is taken once at a dose of 100–150 mg. If there is no effect, a repeat dose of 100–150 mg is prescribed after 5 days. It should be especially emphasized that, unlike other antibiotics, a single oral dose of fungolon can achieve a therapeutic effect in 90–100% of cases.
Sanitation of foci of extragenital infection is carried out taking into account the sensitivity of pathogens to antibacterial drugs.
Planning and preparation for pregnancy is possible only with persistent and long-term (more than 6 months) remission of the herpes viral infection, as well as after eliminating disorders in the reproductive system, taking into account the main factors of termination of pregnancy. An important condition for proper preparation for pregnancy is the normalization of the immune and interferon status of patients using enzyme therapy. Since almost any infection is accompanied by disruption of energy and metabolic processes at the cellular, tissue and organ levels of the human body, preconception preparation should also include metabolic therapy. In this case, a complex of drugs is used that stimulate bioenergetic processes in cells and tissues - riboflavin mononucleotide, lipoic acid, calcium pantothenate, tocopherol acetate, riboxin, potassium orotate, pyridoxal phosphate, phytin, troxevasin.
Metabolic therapy is prescribed for 7 days with a 2-3 week break, in the form of complexes. Multivitamin therapy with a complex of microelements is also indicated. Carrying out early diagnosis, prevention and treatment of infectious pathology of the reproductive system of women before pregnancy, preconception preparation and pregnancy planning can reduce the frequency of complications of the gestational period, the severity (frequency and duration of relapses) of the infectious process during pregnancy, prevent severe forms of neonatal infection, and reduce perinatal morbidity and mortality.
Blockade of herpes simplex virus reproduction in episodic or suppressive therapy. Use acyclovir 0.2 g 5 times a day for 5 days for mild infections (exacerbations once every 6–8 months) and 0.2 g 4 times a day continuously for 2–2.5 months - with frequent relapses (exacerbations once every 30–90 days).